*For medical professionals only
What should I do if my children have food allergies?
As an allergic person, the author found himself some time ago after eating apples will appear laryngeal obstruction, in the past after eating apples have not appeared such a situation, at first simply thought which apple is too acidic, until I ate apples every time I had this laryngeal obstruction feeling, after going to the hospital to check the allergens, I realized that I was allergic to apples.
In daily life, many parents will also find similar experiences in their children, children suddenly have allergy symptoms, such as rashes, diarrhea, vomiting, feeling difficult to swallow, etc., after checking various reasons, it is found that it is because eating a certain type of food leads to allergic reactions. How do we address this situation? Do you not eat this kind of food at all, or do you have another trick?
Food allergies are a problem for many families
According to statistics, about 30%-40% of the world's population is currently plagued by allergic diseases. In young children, the incidence of food allergies is increasing year by year. In Europe and the United States, about 8% of children are affected by food allergies [1].
What we say about childhood food allergies on a daily basis includes types of IgE-mediated, non-IgE-mediated, and mixed types, of which IgE-mediated food allergies are types of acute exacerbations. Simply put, when the body's immune system recognizes that certain foods are harmful to the body, the immune system begins to attack these foreign "invaders", causing our body to develop a series of symptoms of allergic reactions.
The risk factors for food allergies can be broadly divided into the following categories:
1. Genetic factors
Many studies now tend to attribute the high incidence of allergies to heredity. If someone in the family has a food allergy, especially if the mother has a history of food allergy, then the next generation also has a greater chance of developing a food allergy.
2. Environmental factors
An environment that is too clean can be more likely to cause your child to develop allergy symptoms, which may be related to the flora we are exposed to in our daily lives. Studies have found that exposure to more flora can effectively improve children's immunity, more contact with nature, play with mud, tread grass is a very good choice.
However, it should be noted that when air pollution is polluted, it is necessary to avoid going out, because polluted air will increase the occurrence of allergies.
3. Breastfeeding
Short breastfeeding time is likely to make children more prone to allergies, which is likely to be related to breast milk, especially colostrum, which is rich in A immunoglobulins and various nutrients required by infants, which can help young children avoid allergies.
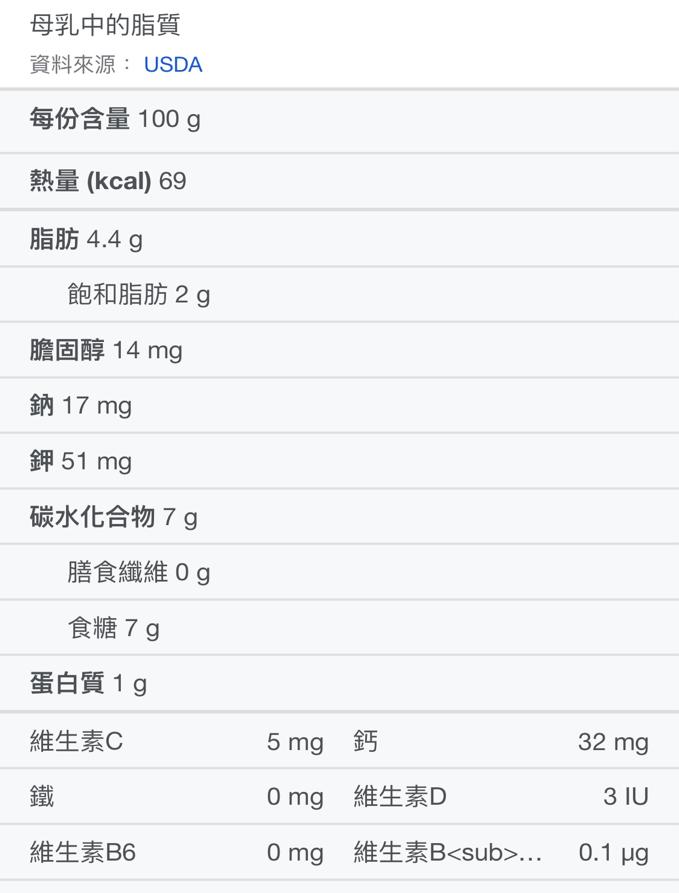
Nutritional composition list of breast milk
It's sometimes really hard to completely circumvent allergic foods
Many parents find that their children are allergic to a certain food, so that the food basically disappears from the family table. But sometimes, children will still eat foods that cause allergies, resulting in severe allergic reactions.
In an ordinary family in the United States, the biggest challenge that housewife Kim Yates Grosso faces every day is how to keep her daughter Tessa safe. Tessa is acutely allergic to milk, wheat, eggs, nuts, aquatic shellfish and many other foods, and even spilling milk on her skin when she was a toddler could cause anaphylactic shock.
Protecting Tessa from food allergies every day is mom's most important job, and she even applied to the government for a professional nurseryman to take care of her daughter during the day, but such a "copper wall" did not bring foolproof. When Tessa was 7 years old, he was sent to the rescue room because of a Vietnamese rice roll, and the staff mistakenly thought that the rice roll was made of rice flour, but did not think that the main ingredient of the rice roll was wheat, which led to Tessa's severe allergy.
After this incident, Tessa, although rescued (using large doses of hormonal drugs), developed panic disorder, refused to go to school alone, and wanted to be with her mother all the time, and even refused to eat when there was no mother. Father Kim knew that things could not go on like this any longer, and that not eating for a while would not solve all problems, so they sought treatment from a specialist.
Experts have given the answer, in order to live a normal life in the future, it is necessary to carry out desensitization treatment, try a treatment called "oral immunotherapy", which is to give allergy patients a small dose of allergens every day, gradually increasing over several years, slowly "re-educating" the patient's hyperinfluous immune system, until the patient finally establishes tolerance to this food, it is no longer dangerous.

Pictured: Tessa undergoes desensitization treatment. Source: https://www.today.com/parents/hope-deadly-childhood-allergies-one-moms-journal-clinical-trial-1c8853538
Tessa began oral immunotherapy, starting with a powder of 1 mg, increasing the dose every two weeks until a year and a half later. Tessa became more and more cheerful, and after the last dose of allergen powder, Tessa ate a whole serving of eggs, wheat, milk, peanuts, and almonds. She ate them, an hour passed, two hours passed, and then she was safe.
Is it safe to "attack poison with poison"?
Many people must have questions, is the above treatment really effective and safe?
In the United States, about 2 percent of children are allergic to peanuts, or nearly 1.5 million children under the age of 17. The risk of fatal allergic reactions from accidental consumption of peanuts is enormous for these children, most of whom have been allergic to peanuts throughout their lives.
So a clinical trial funded by the National Institutes of Health found that oral immunotherapy for children with peanut allergies between the ages of 1 and 3 could desensitize most of them to peanuts, and one in five children had peanut allergy symptoms relieved. The results of the trial, called IMPACT, were published in the journal The Lancet.
Source: Literature[3]
A total of 146 children aged 1 to 3 participated in the trial, and these children developed allergic reactions when consuming 500 mg of peanut protein or less. The children were randomly assigned (2:1) to either a peanut protein-containing powder or a similar-looking placebo powder, with no difference in taste.
Initially, the amount of peanut protein consumed by the children in the treatment group gradually increased each day, starting with a small dose and gradually increasing the dose until 2 grams (about 6 peanuts). Over the next two years, they gradually increased the dose of peanut protein until they accumulated up to 5 grams (about 16 peanuts). Then let the child not eat peanuts for 26 weeks.
After 26 weeks the children were challenged with 5 grams of peanut protein and were given 8 grams of peanut oil (about 2 tablespoons) the next day to the children who did not have an allergic reaction during the challenge to confirm that they would not have an allergic reaction when eating peanuts. After the trial, the organization defined peanut allergy symptom relief as being able to consume at least 5 grams of peanut protein six months after immunotherapy was completed and there was no allergic reaction.
By the end of the treatment period, 71 percent of children treated with peanut flour had been desensitized to peanuts, compared with only 2 percent of children treated with placebo flour. During the 2-and-a-half-year treatment period, 21 children received rescue drug treatment (epinephrine) for a moderate response to peanut flour.
From the above experimental results, it is not difficult to see that oral immunotherapy is effective and relatively safe, previous studies have proved that the younger the child, the better the effect, it is recommended to start oral immunotherapy for children aged 1 to 3 years old, but this does not mean that the child has no meaning after aging.
Taking the author as an example, after being allergic to apples, I underwent "desensitization treatment" on myself, because I think apple juice and apple pie are so delicious, if you give up, life will be less fun. So I began to consume a small amount of apples every day, but not accurate to grams, from the size of the knuckles of the little finger to the size of the thumb, after my continuous efforts, I could eat the apple again, but I found that I was starting to be allergic to pears...
While my apple desensitization was a success, I would like to remind you that desensitization treatment is still a significant risk because of the lack of standardized allergen intake and allergen introduction methods. The reason why I dare to try desensitization treatment at home is that first of all, my allergy symptoms are not particularly serious, and secondly, I am a doctor and an allergic constitution patient, and I have hormone drugs at home in case of emergency.
Therefore, if the child wants to desensitize treatment, be sure to communicate with the doctor before implementation, and do not feed the child the food that will cause allergies without guidance.
bibliography:
[1] Gupta RS,Springston EE,Warrier MR,et al. The prevalence,severity,and distribution of childhood food allergy in the United States.Pediatrics 2011;128:e9.
[2] Roslund M I,Puhakka R,Gr nroos M,et al. Biodiversity intervention enhances immune regulation and health-associated commensal microbiota among daycare children[J]. Science Advances,2020,6(42):eaba2578.
[3] Prof Stacie M Jones,Edwin H Kim,Prof Kari C Nadeau et al. Efficacy and safety of oral immunotherapy in children aged 1–3 years with peanut allergy(the Immune Tolerance Network IMPACT trial):a randomised placebo-controlled study Published:January 22,2022DOI:https://doi.org/10.1016/S0140-6736(21)02390-4
This article was first published: Pediatrics Channel of the Medical Professions
This article is written by Cao Gongzi
Editor-in-Charge: CiCi