At this moment, after experiencing repeated defeats and collapses after a month of robbing the Shenzhen isolation hotel at 10 o'clock every day on time and brushing the tickets of the Hong Kong-Zhuhai-Macao Bridge every Tuesday, the author took the CX986 flight from Hong Kong to Chengdu, began to isolate, and the curve went back to depth.
Since returning to Hong Kong on January 27, the author has almost completely experienced the fifth wave of the Omicron epidemic in Hong Kong, from dozens of days, to hundreds, to thousands, to tens of thousands, to tens of thousands, and then to today's "fact lying flat". At the same time, the mainland is also facing the high challenge of Omicron, and the number of new infections in Shanghai today has exceeded 1,600, and the number of new infections in the country has increased by about 5,000 for many consecutive days.
Hong Kong's "sit-ups" between "lying flat" in Europe and the United States and "standing firm" in the mainland have become a good data reference for supporting the mainland's epidemic prevention policies.
This article speaks with data and is ready to answer the following questions in two phases:
Previous issue:
1. As of now, how many people have been infected in Hong Kong?
2. What is the typical pathogenesis of Omicron?
3, is the death rate of Omicron in Hong Kong really high?
4, Are Omicron's after-effects terrible?
Next Issue:
5. How to carry out home anti-epidemic and prepare what necessary materials?
6, why has Hong Kong repeatedly postponed the national nucleic acid testing, and where is the tipping point between doing and not doing?
7, Why can Only Hong Kong do sit-ups?
8. Is Hong Kong the culprit in the current round of epidemics in the mainland? Hong Kong has decided to continue to liberalize, what will happen to the mainland?
9. What is the significance of the fifth wave of the epidemic in Hong Kong for the adjustment of prevention and control in the mainland?
Q1 How many people have been infected in Hong Kong so far?
According to official data released by the Health Care Centres and Hospital Authority of the Hong Kong Department of Health, as of 24 March, the total number of confirmed cases of the fifth wave of the epidemic exceeded 1,088,593, of which 698,253 cases were confirmed by nucleic acid testing and 390,340 cases were reported after rapid antigen testing. With a total population of 7,394,700, the proportion of infected people is 14.72%.
As of 24 March, the number of confirmed cases and population of the fifth wave of Omicron outbreak in Hong Kong (by age group)
Notably, Omicron hits all ages indiscriminately. Among the various age groups, the infection rate (the number of people infected in this age group ÷ the number of people in this age group) is between 8% and 16%, and the difference is very subtle, which is very different from the characteristics of the early "new crown virus mainly attacking the elderly". Middle-aged people between the ages of 20 and 60 have even slightly higher infection rates than children and the elderly, which is related to their social range.
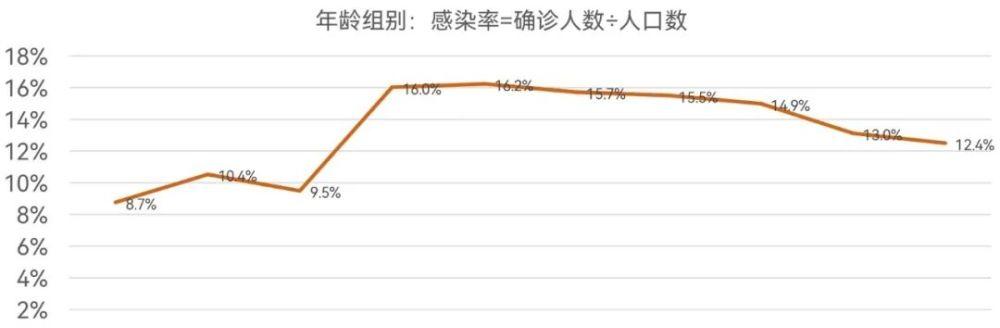
Infection rate of the fifth wave of Omicron outbreak in Hong Kong as of 24 March (by age group)
Although this data looks big, it is still just the tip of the iceberg. So far, Hong Kong has not carried out even one round of national nucleic acid testing, and the official cannot grasp the real situation, and the situations that are not included in the statistics include:
1. The person who receives the compulsory test order does not cooperate with the compulsory inspection or forgets to go to the compulsory inspection.
The author's community was tested positive for the environment due to the sewage pipe after the Spring Festival, and it was immediately included in the enclosure and compulsory inspection. Although the enclosure was only one night and could be released early the next morning, there were still many families knocking on the door without answering, whether it was really no one at home or did not want to cooperate and could not be identified. At the same time, Hong Kong has strict protection of personal privacy, and has not released unanswered family information, and finally after testing 3 positive patients that night, it was completely unblocked the next morning. For another example, the Hong Kong version of the place code - safe travel, in the early stage of the epidemic, also issued mandatory testing for people who intersected with the confirmed patients, but the mandatory inspection notice was only a text message, many people did not see it, and some people saw it and forgot to test, and finally it was gone. It is unimaginable in the mainland to force inspections without inspections, but why is it so "arbitrary" in Hong Kong involves the issue of the so-called coercive power of the government, which will be analyzed separately later.
2. Self-rapid antigen test is positive, but is not reported to the government.
Rapid antigen testing, which has just been liberalized in the mainland, has been listed in Hong Kong for a long time. Since the fifth wave of the epidemic, it is believed that almost every household has a rapid test kit, and the government is also distributing rapid test kits for free. According to the requirements of the government, people who test positive for themselves should report through a special website. However, as of now, the reported cases of "national self-inspection" instead of "national compulsory inspection" are only 390,000 cases, far lower than the nearly 700,000 cases of nucleic acid testing, and it is obvious that the data deviation is very large.
Why are people who test positive for themselves reluctant to report to the government? This problem has very important reference value for the mainland that is implementing self-antigen testing.
First of all, the vast majority of Omicron are asymptomatic infected people (released in Shanghai on March 25 today: 29 confirmed cases, 1580 asymptomatic infected people) and mild patients, the former does not need treatment, the latter according to the cold symptomatic medicine (such as Bi Li Tong, paracetamol, Lotus Qing plague, etc., go to the hospital is also these drugs) can be cured and turn negative. As long as the family has a separate room to arrange for patient isolation, there is no incentive to report, because reporting does not bring additional benefits to the patient and the family, but rather brings more restrictions, including: may be sent to a worse condition of the cabin, the other members of the family (defined as close contacts in the mainland) of the ban, and so on. Second, if a self-test-positive patient is not reported, it is practically impossible for the government to trace the behavior, because the self-tester can claim that he has not self-tested, so he does not know that he is positive. Again, even if reported, due to the large number of people diagnosed in the early stage, the government actually has no more resources to quickly follow up and deal with this large number of asymptomatic and mild patients, but after the report, it automatically replies to a text message to express "received", and then sends a medical package to the home address within a few days, but many people said that when the medical package is received, the symptoms are almost better. In summary, if the self-test is positive and reported to the government, there is no legal compulsion (nor can it be enforced), no additional benefits, just increase the restriction out of thin air, then it is all up to self-awareness. Similarly, after the rapid self-examination of open antigens in the mainland, how to ensure positive active reporting is also a problem.
3. Asymptomatic infected and mildly ill people who have not been tested.
As mentioned earlier, so far, Hong Kong has not done compulsory nucleic acid testing for the whole people, and asymptomatic infected people will not do rapid antigen testing on their own when they are completely unaware. For mild patients, as long as there are no elderly and children in the family who need protection, many young people just have a sore throat, not even a fever, and may not be tested.
Since government data is distorted, is there any more credible data? On March 22, the University of Hong Kong School of Medicine gave the latest mathematical model calculations, and as of March 20, the number of infected people was as high as 4.4 million, accounting for 60% of the total number of people in Hong Kong.

Source: March 22, Kodai University School of Medicine
Is this data credible? Since the press conference has only been a few days, the government has not yet commented on it. But the last time (15 March) the Faculty of Medicine of HKU made an estimate of 3.58 million people infected, the Infectious Diseases Division of the Center for Health Protection considered the estimate reasonable and said that behind every 1 infected person found, there may be 3 to 4 unidentified people.
From the author's circle of friends in Hong Kong, if you take the family as a unit, about half of your friends have been recruited. Considering the author's circle of friends, one is that the mainlanders are the main ones, who are afraid of the new crown; second, there are children at home, and they are worried about aggravation; third, there are no seven aunts and eight aunts in Hong Kong, and the social relationship is simple, which should be regarded as the offline epidemic. Therefore, 60% is a reliable percentage of recruits.
Video source: Hong Kong 01
60% of the number of infected people, whether it is the course of the disease, death, sequelae and other issues, have the basis for data analysis, and then discuss them one by one in three questions.
Q2 What is the typical pathogenesis of Omicron?
The "wild strain" of the new crown virus that created the first wave of the epidemic in Wuhan has brought too shocking memories to everyone. But the new crown entered its third year, and after many rounds of mutation, it was also learning to coexist with humans. The purpose of the virus is not to kill the host, after all, the host is dead, it is also dead. According to the laws of natural evolution, in order to allow the virus to multiply from generation to generation, its optimal strategy is to reduce toxicity and increase transmissibility. Thus, evolved to the current Omicron variant.
The following figure shows a schematic diagram of the pathogenesis process that has been widely circulated during the epidemic in Hong Kong. There are not a few friends recruited by the author's side, and without exception, they have completed the whole process from infection to yin according to this, and the difference in the middle is to advance or postpone it for a day or two.
Very reliable Omicron's course of development
Days is the timeline that represents the number of days, where D0 is the day of infection.
The Infectiousness curve indicates infectivity, and the higher the curve, the more contagious it is.
Symptoms ribbons indicate symptoms, and the darker the color, the more pronounced the symptoms.
D1-D3: Incubation period. Patients gradually begin to feel, usually manifested by discomfort in the throat. However, at this time, the rapid test is still negative, and the patient cannot tell whether it is a normal throat discomfort or a stroke. Fortunately, the infectivity at this time is also very low, otherwise the infectivity of Omicron would have increased by leaps and bounds.
D4-D6: onset of illness. The course of the disease has entered a period of rapid development. If the autoimmune system defeats Omicron at this time, congratulations, you have become an asymptomatic infected person; if the immune system does not resist this wave of attack, the patient begins to have fever, cough, sore throat, muscle soreness and other symptoms, and the mild patients basically reach the peak of discomfort in D6; severe patients will be very unwell at this time and need to be sent to the hospital for treatment, which is beyond the scope of this discussion. As the course of the disease deepened, the antigen concentration also began to be obvious, and the rapid antigen detection gradually changed from a light T line of D4 to a dark T line of D6.
D7-D10: Rehabilitation period. The vaccine has trained the immune system for several rounds, gradually defeating Omicron, starting with D7, gradually disappearing symptoms, and sometimes even forgetting to take medicine. The patient's physical discomfort is slowly replaced by the psychological discomfort of isolation, and they are eager to test once an hour to see if it turns negative. D9-D10, basically can turn negative. After two consecutive days of clouding, the infectivity has basically disappeared, and according to hong Kong rules, it can be lifted from isolation and returned to normal life. There are many cases, in D8 or D9, the color of the T line is still relatively dark, but it may disappear suddenly after one night, there is no process of gradually lightening the color, so the patient should not be anxious because the color is not lighter.
In summary, the discomfort of Omicron was concentrated in D3-D7 for a total of 5 days, the infectivity was concentrated in D4-D9 for a total of 6 days, and the antigen-positive test was concentrated in D4-D10 for a total of 7 days. You can compare yourself with the cold, and the conclusion is self-evident.
Q3 Hong Kong Omicron mortality rate is very high, is it true?
First of all, I would like to state that the author was not born as a medical professional, and the following discussion is based on common sense (Common Sense), and if it is not correct, please judge for your own judgment.
As of 24 March, the fifth wave of the Omicron outbreak in Hong Kong had a total of 6,557 deaths, a mortality rate (number of deaths/total population) of 0.08%, that is, 8 deaths per 10,000 people, a case fatality rate (number of deaths/number of infections) of 0.6%, and 60 deaths of 10,000 infected people. No wonder, Dr. Zhang Wenhong said on March 14 on the Huashan Infection Official Micro that in countries that have achieved extensive vaccination and natural infection rates, the case fatality rate of the new crown virus has been lower than that of influenza.
Source: Hong Kong Department of Health, COVID-19 Wave 5 Data
However, if we carefully study the situation of the elderly over 80 years old, it can be clearly seen that the mortality rate is 1.2%, that is, 1.2 deaths per 100 people over the age of 80, and the case fatality rate is as high as 9.3%, that is, almost 1 person will die for every 10 infected people over the age of 80. It should be said that this is the most concerned point of the media in this round of the epidemic, and it is also the point where the high case fatality rate in Hong Kong is most criticized.
There are several important concepts that must be explained in this regard, otherwise it is of little significance to say that the high case fatality rate is generally high.
First of all, dr. Zhang Wenhong had an important premise when saying that the case fatality rate of the new crown was lower than that of influenza, that is, to achieve widespread vaccination and natural infection rate. Unfortunately, the first four waves of the epidemic in Hong Kong were very well controlled (very low freedom restrictions, rapid dynamic clearance), which on the one hand made the natural infection rate low, and on the other hand, made the elderly think that the risks of vaccination may outweigh their benefits. At that time, Hong Kong was dominated by the mRNA vaccine Fu bi thai and the inactivated vaccine Coxing Biologics. For the former, the society generally believes that there are unknown risks, which are not conducive to the vaccination of the elderly and children, while for the latter, it largely continues the consistent prejudice against the mainland, believing that Kexing Biology does not have much effect. The end result is that neither is played. Therefore, dr. Zhang Wenhong's premise no longer exists, no matter what age, 60%-70% of the deaths have not been vaccinated, about 20% have only been vaccinated, and the whole process of vaccination has not been completed, and the total of the two situations accounts for about 80%-90% of the deaths.
So, the point is, needles! injection! injection!
Source: Hong Kong 01
Secondly, deaths over the age of 80 account for 70% of all deaths in Hong Kong, which can be called the vast majority. Unfortunately, the author did not get the specific age of cases over 80 years old, only know that the minimum age is 80 years old, the average age is not clear, can only be conservatively considered to be about 85 years old. Interestingly, hong Kong's 2021 life expectancy ranking released by UN-Habitat is the highest in the world, at 85.29 years. Therefore, it is obvious to conclude that the conservative average age of death, which accounts for the vast majority of deaths in Hong Kong, is very close to the life expectancy of Hong Kong itself. The implication behind this is difficult to say but obvious.
Third, the statistics of COVID-19 deaths actually include three types of people. The first type is called death of the new crown (die of), that is, directly in the clinical death of the new crown virus; the second type is called death with poison (die with), that is, the cause of death has nothing to do with the new crown virus, but at the same time the body is detected with the new crown virus, such as falling from the building, stroke and other people, after admission to the hospital found positive, but no new crown disease. Of course, these two categories are sometimes difficult to judge, so the reason for the third category is temporarily unknown.
Hui Shuchang, an expert consultant to the Hong Kong government and chair professor of respiratory system at Chinese University, analyzed 120 cases of the fifth wave of deaths and concluded that the proportion of deaths from COVID-19 and death with poisoning was 38% and 37% respectively, almost the same. This is also a major interesting conclusion in the current COVID-19 statistics.
In summary, Omicron is already a mild virus, and everyone no longer needs to look at the current epidemic situation in Wuhan in the early stage of the new crown, otherwise it is a sword. Viruses are evolving, but what about people?
Q4 What are the sequelae of Hong Kong Omicron?
Human beings are afraid of viruses in two ways, one is the pain and even death of the disease process, and the other is the long-term sequelae that may result after the disease is cured.
Regarding the first aspect, as mentioned above, the vast majority of people are asymptomatic and mild, and the process of getting sick is neither painful nor easy to die. That's a reason to continue to think of him as an extreme Case, and only the aftermath remains.
The Omicron virus only began to circulate in the second half of 2021, and Hong Kong only began to erupt during the Spring Festival of 2022. So, with a simple logic, most of the current research on the sequelae of the new crown virus is either not aimed at the Omicron variant or has just begun.
A typical example of the former is the recent oxford paper "SARS-CoV-2 is associated with changes in brain structure in UK Biobank", published in the journal Nature. This is an intriguing topic, covid-19 is related to changes in the structure of the human brain! For a time, various interpretations of the public number hustled and fell, and used this to explain why the new crown will lose taste and smell, because the brain nerves in these two areas are damaged. But a closer look at the article shows that the time point of the article to collect brain imaging data from new crown patients is April 2021, when the Delta strain was popular in the UK, and this part of the patients should be infected with the previous Alpha, Beta, and Gamma variants, and Omicron is almost certainly not among them.
For the latter, at least in Hong Kong, it has only recently turned cloudy, and there is no clear data. Sequelae do not occur out of thin air, and must be related to the damage to the body at the time of onset. A large number of asymptomatic infected people indicate that autoimmunity has nipped Omicron in the bud, and it is even more difficult to imagine that it can also have delayed lethality. In terms of the clinical manifestations of mild patients, Omicron mainly attacked the upper respiratory tract and did not attack the lungs, so in Hong Kong, Omicron was jokingly called "new crown upper respiratory tract infection", rather than "new crown pneumonia", since the lungs were not damaged, it is difficult to imagine the possibility of subsequent damage. As for some recovered patients who have shown in interviews with the media that their physical fitness decline, inattention, anxiety, poor memory, and changes in sleep habits, I just want to say that eating and drinking during the Spring Festival, coupled with more than 10 days of home isolation, even a good person will also have these "sequelae". If you study the sequelae of children's daily online classes on the computer, I am afraid it is even worse than this; and then study the author's two-place family, the real sequelae to want to die! Again, the author was not born in medicine, and the following are personal understandings. I want to emphasize that Omicron's sequelae are still lacking in research, and the current exaggeration is not really a scientific conclusion.
About author:Yan Jingyu, Ph.D., University of Chinese, Hong Kong, Executive Vice President of Galaxy Industry Group, Partner of Galaxy Capital. He once worked at the Chinese University of Hong Kong and the Shenzhen Municipal Development and Reform Commission, responsible for the planning and construction of 23 strategic emerging industry base agglomeration areas in Shenzhen, participated in the formulation of the economic policies of The Headquarters of Shenzhen, and is currently responsible for the management and operation of galaxy WORLD Park, and invested in yuncong technology, taihe water, delicious and other enterprises, interstellar glory, national star aerospace and other enterprises.