Mr. Li, 42 years old, who is slightly fat, suddenly suffered a heart attack and put a stent. Postoperative re-examination of dyslipidemia (LDL-C 4.68 mmol/L) requires lipid-lowering and anticoagulation.
Mr. Li is more confused, why should I control blood lipids infarction? How to lower blood lipids? What tests do I need to do? How low do you want to control?
What are lipids?
Lipids (lipids) are a general term for lipids (lipids) contained in plasma, including total cholesterol (free cholesterol and cholesteryl esters), triglycerides (TG), free fatty acids (FFA), phospholipids, glycolipids and so on.
There are two sources of lipids, exogenous lipids are ingested into the blood from food, and endogenous lipids are synthesized by liver cells, fat cells and other tissue cells into the bloodstream.
Lipids are affected by diet, age, sex, occupation, and metabolism, and fluctuate widely.
Lipids are insoluble in water and usually bind to apolipoproteins to form lipoproteins, which can only be transported and metabolized in the blood. Because the types and contents of lipids and apolipoproteins contained are different, the density, size, surface charge, physiological function, etc. of lipoprotein particles are different.
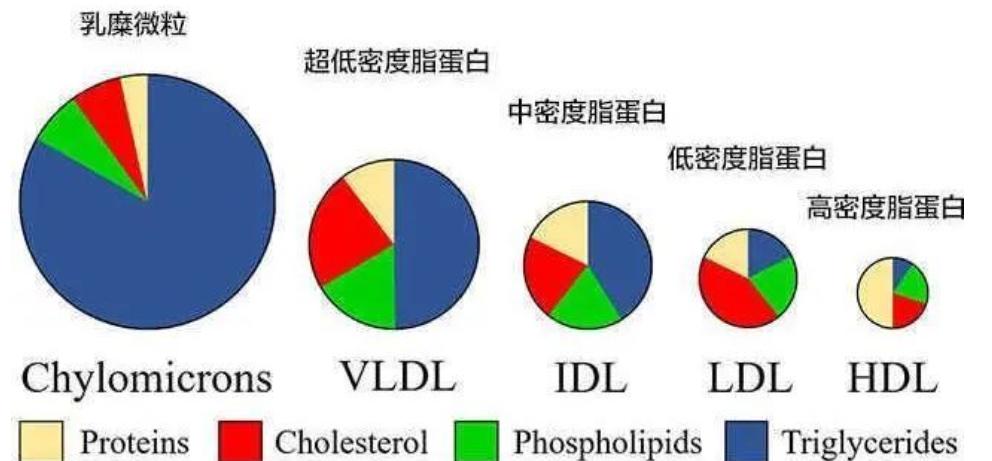
Clinically, according to the density of lipoprotein, it is divided into five forms: chylomicrons, very low density lipoprotein (VLDL), low density lipoprotein (LDL), medium density lipoprotein (IDL), and high density lipoprotein (HDL).
What are the functions of the five lipoproteins?
Chyle particles are mainly responsible for the transport of exogenous triglycerides and cholesterol; very low-density lipoproteins are mainly responsible for transporting endogenous triglycerides; LDL is mainly responsible for transporting endogenous cholesterol; hdL cholesterol is mainly responsible for reverse transport of cholesterol, which produces cholesterol from extrahepatic tissue cells, which is transported to the liver through blood circulation and converted into bile acids through liver metabolism.

Are blood lipids transported through lipoproteins needed by the body?
Lipids are indispensable substances in human life activities, such as triglycerides are important energy substances of the body; cholesterol, phospholipids and glycolipids are important components of biofilms, involved in cell recognition and signal transduction, or precursors of a variety of bioactive substances; fatty acids will be metabolized to produce fatty acid derivatives also have important physiological functions.
Lipids are so important, why control lipids?
Blood lipids are indeed essential substances in our human life activities, but high blood lipids can cause harm to the human body (especially human blood vessels). For some people at high risk of cardiovascular disease, even normal blood lipid levels can cause damage to human blood vessels.
Human health faces two major chronic diseases: malignant tumors and cardiovascular and cerebrovascular diseases. According to the World Health Organization, cardiovascular disease is the most important cause of human disease death. Therefore, attention must be paid to vascular health. There are many factors that affect vascular health, including age, sex, smoking, high blood pressure, diabetes, dyslipidemia, and family history of cardiovascular disease.
A large number of randomized clinical studies have confirmed that elevated low-density lipoprotein cholesterol (LDL-C) is a key factor in the formation of atherosclerosis, and reducing LDL-C levels can significantly reduce the risk of morbidity and death of atherosclerotic cardiovascular disease (ASCVD).
What are the contents of the lipid test?
Regular examination of blood lipids is an important measure for the prevention and treatment of dyslipidemia and cardiovascular disease, not only for distinguishing whether blood lipids are normal, but also to predict and assess the risk of cardiovascular disease in the population, and to guide lipid intervention and treatment.
Blood lipid programs generally include four basic items: total cholesterol, triglycerides, LDL-C, and HDL-C. Other projects that are receiving increasing attention include the following:
Lipoprotein a(Lp(a))
Its elevation is common in ASCVD, acute myocardial infarction, diabetes and other diseases, and the low point is good!
Apolipoprotein A (ApoA)
It is the main ingredient of HDL-C, and the high point is good!
Apolipoprotein B (ApoB)
Simultaneous measurement with LDL-C facilitates clinical judgment. Low point good!
How often should lipids be measured? Focus?
In order to detect dyslipidemia in a timely manner, it is recommended that:
1. Adults aged 20-40 years are measured at least once every 5 years;
2. Men over 40 years old and women after menopause are tested for blood lipids every year;
3. Patients with atherosclerotic cardiovascular disease and their high-risk groups should be measured once every 3-6 months.
4. Patients hospitalized due to atherosclerotic cardiovascular disease should be tested for blood lipids at the time of admission or within 24 hours of admission.
The focus of blood lipid monitoring: people with a history of ASCVD; people with high incidence of ASCVD such as hypertension, diabetes, obesity, and smoking; people with a family history of early-onset cardiovascular disease; patients with familial hyperlipidemia; xanthelasma of skin or tendons and thickening of the Achilles tendon.
How to understand the different reference and control ranges of LDL-C?
The reference range for LDL-C on the test form is based on the measurement values of the vast majority of normal populations, but for specific individuals, it is more valuable to set specific LDL-C control goals based on the risk level of cardiovascular accidents.
Populations with different risk levels require very different LDL-C/non-HDL-C target values (see table below). If your cardiovascular accident risk level is low/moderate, you can simply control LDL-C below 3.4 mmol/L, but if you are in a very high-risk group, it is recommended that you control blood lipids more strictly and reduce LDL-C to less than 1.8 mmol/L.
How to control blood lipids?
Lifestyle changes
Dyslipidemia is closely related to lifestyle. Whether or not medications are chosen, lifestyle modification is the preferred option for lipid control.
A good lifestyle includes: controlling dietary cholesterol intake; increasing physical activity; maintaining an ideal weight; and staying away from risk factors such as tobacco.
Pharmacological interventions
Actively lowering blood lipids and timely drug intervention are also important means. At present, the lipid-adjusting drugs commonly used in mainland china mainly include statins, fibrates, niacin and cholesterol absorption inhibitors. Among them, statins are the most widely used in clinical practice.
summary
LDL-C is an atherosclerotic lipoprotein;
Reducing LDL-C is the main intervention goal for reducing cardiovascular risk;
Lifestyle improvement, statin therapy are the main means of lipid lowering;
Strengthen the concept of blood lipid management to ensure blood vessel health.
Source: Second Courtyard of Zhejiang University
Edited by: Yeah Reviewer: Xiao Ran