term
abbreviation
GO OUT
definition
Chronic progressive systemic inflammatory diseases that predominantly involve joints
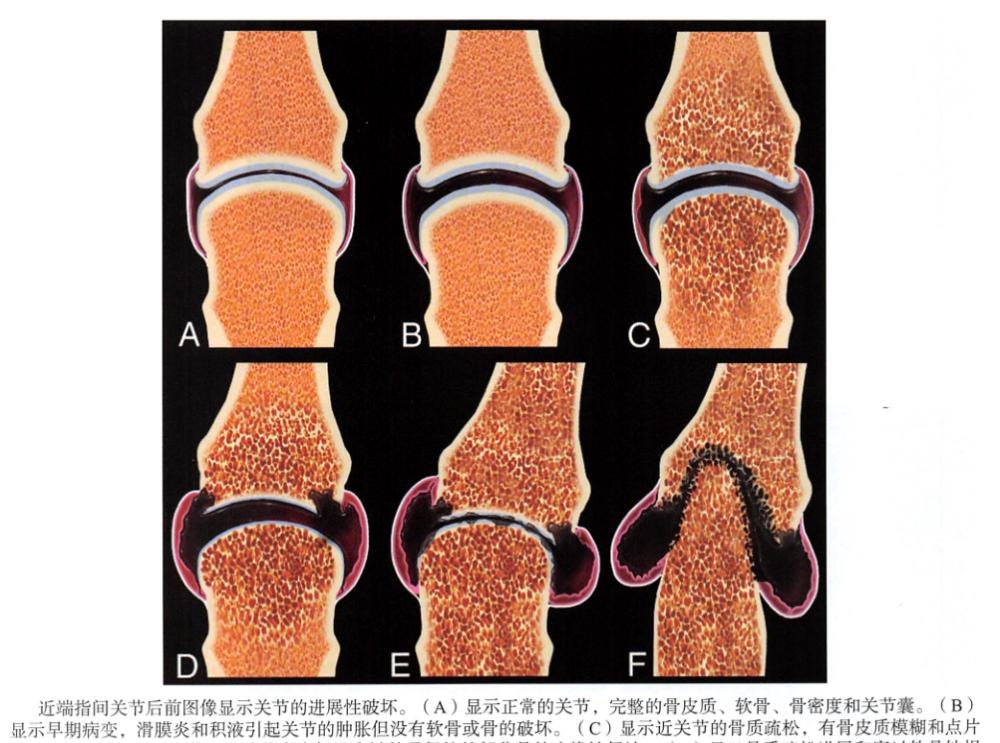
image
General performance
The best diagnostic basis
Simple erosive lesions
osteoporosis
The arrangement is not neat
place
Typical symmetrical lesions
Early stages of the disease can be unilateral
Site of early involvement of the lesion
Metacarpophalangeal joints
Distal radial joint
Radial wrist joint
Site of late involvement
Proximal interphalangeal joint
Inter-carpal joints
Note: Distal interphalangeal joints are almost unencumbered
X-ray performance
Hands and feet are affected at the earliest, pay attention to minor changes
Localized soft-tissue swelling may indicate underlying bone involvement
In particular, the metacarpophalangeal joint, proximal interphalangeal joint, and ulnar stem process
osteoporosis
Early stage: paraarticular
Late: diffuse
erode
The earliest is the blurring of the bone cortex, and later the loss of the dotted bone cortex
Marginal erosion of bone appears early and is not covered by cartilage in the joint capsule
"Mouse ear" manifestation at the base of the phalangeal bone
The radius and ulnar stems are protruding
Direct subchondral erosion
Severe destruction of bone structures in the late stages
The phalanges may have a "pen cap" performance
The arrangement of the distal ulna or proximal carpal bone can be disrupted
Destruction of cartilage
Initially the x-ray is swollen due to standing water, and the joint space appears to widen
Thinning of cartilage and narrowing of the joint space are consistent
Subchondral cysts are common in rheumatoid arthritis
The ulnar stem process can appear "cap-shaped": the only site of proliferative lesions in rheumatoid arthritis
Ligaments or tendons are torn and caused by an insordination
Armbone
Ulna displacement (carpal bone subluxation toward the ulnar side causes the lunar bone to be almost connected to the ulna)
The radial radius of the carpal bone is subluxed towards the metacarpal side
Separation of the moon bones
Palmar or dorsal segmental instability (VISI or DISI)
finger
The ulna is displaced toward the metacarpophalangeal joint
Metacarpophalangeal subluxation
"Thumbs up for a ride"
Button-like (hyperflexion of the proximal interphalangeal joint, hyper-dorsal distal interphalangeal joint) and gooseneck (excessive dorsal proximal interphalangeal joint and overflexion of the distal interphalangeal joint) malformations
CT findings
Consistent with x-ray findings, it is rarely used except for postoperative evaluation
MR performance
T1 weighted image
Low signal of fluid accumulation and erosion
Liquid-sensitive sequence
High-signal effusions, erosions, subchondral cysts
Hyperinfactory tenosynovitis
Vascular filament: Thick, nodular low-signal synovial membrane surrounds the effusion
Bone marrow edema: hyperintensity under the cartilage
T1WI fat pressing intensification
Thickened, visibly strengthened synovial membrane, lining up low-signal fluid build-ups and erosions
Tenosynovitis: strengthening of the tendons involved
If tenosynovitis of the carpal tunnel involves the median nerve, the median nerve may be strengthened
Ultrasound performance
Early effusions of small joints are well explored
Tenosynovitis: High-turn voice
Tendon tear: can be seen directly
Color Doppler evaluates vascular hyperplasia
Rheumatoid nodules: uniform high-signal masses
Imaging methods
Optimal imaging method
The initial imaging is X-ray imaging
If negative, MAGNETIC resonance is beneficial for the detection of early lesions
Follow-up treatment (usually medication)
Ultrasound Doppler is indicated for effusions and inflammation
MrI is best suited for follow-up of early lesions
Imaging recommendations
Plain: posterior anterior position, large irradiation field
Large irradiation fields are beneficial for the detection of early erosion of the palmar joint, triangular bone, and bean-like bone
If carpal arrangement needs to be evaluated, a lateral positional film should be added
differential diagnosis
Systemic lupus (SLE)
The same form of deformity, but can be reduced
Non-erosive until the end of the disease
Erosive osteoarthritis
Erosive, but has the characteristics of osteoarthritis distribution
Distal interphalangeal joints > proximal interphalangeal joints; 1st wrist metacarpal joint, small polyangular bone of the scaphoid bone, mostly bone joint
Psoriatic arthritis
It may start out as purely erosive
Distribution is most common in distal interphalangeal joints but may involve other joints
The distribution of the carpal bone is unpredictable
There may be manifestations of periostitis (fluffy periosteal reactions around the base of the diaphysis or phalanges)
Hyperparathyroidism
Subchondral bone resorption of the terminal phalanges or collapse of the carpal bone can stimulate erosion destruction
Other manifestations of hyperparathyroidism: subchondral bone resorption, vascular calcification
Polycentric reticular tissue cell hyperplasia
Erosion of the metacarpophalangeal joints at the distal end is pronounced
Osteolysis of the extremities
Soft-tissue nodules can irritate rheumatoid nodules
pathology
General performance
pathogen
The reason is unknown
Pathophysiology is thought to be related to the persistent immune response of a gene-susceptible host to some unknown antibodies
genetics
Genetic predisposition
The consistency of identical twins is 25%
First-degree relatives are 4 times more likely to develop RA than the general population
Individuals cannot have infected family members
General pathology and surgical seeing
Hypertrophy and edema of the synovial lining
Joint swelling, bone erosion, cartilage destruction
Seen in the mirror
CD4 helper T cells, antigen-presenting cells, lymphatic follicle aggregation
A large number of immunoglobulins, including rheumatoid factor, are produced
Synovial neovascularization
Clinical information
Clinical manifestations
Common signs/symptoms
Symmetrical polyarthritis, especially the small joints
Constitutional symptoms: fatigue, low-grade fever
Usually presents with a course of more than a few weeks or months, and occasionally an outbreak of disease
Other signs/symptoms
Wrist and hand deformities
Ulnar displacement of the carpal bone
The bones of the moon are separated, and the wrist joint is unstable
The metacarpal subluxation and the ulnar deviation of the metacarpophalangeal joint
"Button-like", "gooseneck-like" and "hitchhiking thumb" deformities
Ulnar head syndrome
Synovitis ulnar carpal ligament stretching
The dorsal subluxed ulna is exposed to wear and tear of the extensor tendon of the finger
Clinical manifestations: pain, decreased range of motion, dorsal displacement of the ulna
demography
age
The peak incidence is between 30 and 50 years of age
gender
Male: Female = 1: 3
epidemiology
Worldwide incidence of rheumatoid arthritis is 1%
Incidence is 5% in some Native Americans
Wrist joints are involved in 80% of patients with rheumatoid arthritis
85% involve the metacarpophalangeal joint
70% affect the proximal interphalangeal joint of the hand
Outcomes and prognosis
With aggressive multi-drug treatment regimens, most get better
Treatment-insensitive patients show a persistent deterioration of erosion, ligament and tendon lesions
Progressive pain and loss of function
treat
Usually combined with medication, the aim is to relieve pain while rapidly improving the effectiveness of treatment, controlling the disease before the joint is destroyed
Surgical treatment
Synovectomy, tendon sheath removal
Torn tendons often cling to adjacent ligaments
Armbone
Distal ulnarectomy
Proximal carpal bone resection
Articulation fusion (usually the dorsal plate of the radius passes through the sedanular crescent bone, and the skull is fixed to the 3rd metacarpal bone)
Carpal arthroplasty may fail and be complicated by massive osteolysis
Metacarpophalangeal joints, interphalangeal joints
Joint fusion, IP of thumb and finger
Arthroplasty: complications are common
Fracture of the device and fracture of the finger
Massive osteolysis and synovitis
Diagnostic ideas
Think about it
Early rheumatoid arthritis may be monooskeletal or asymmetrical
Must be differentiated from septic arthritis
Key points of image interpretation
Use the swelling of the soft tissues around the hands to guide the discovery of subtle bone manifestations
Note the earliest x-ray signs of erosion: blurred cortical and dotted flaky

This article is excerpted from Non-Traumatic Osteomyoskeletal Diagnostic Imaging
Source: Huaxia Imaging Diagnostic Center
【Copyright Notice】This platform is a public welfare learning platform, reprinted for the purpose of transmitting more learning information, and has indicated the author and source, such as teachers who do not want to be disseminated can contact us to delete