Editor's Note
Pheochromocytoma is a tumor that originates in the chromophilic tissue of the neuroectoderm, 80% to 90% is located in the adrenal glands, mostly occurs in people aged 20 to 50 years, and has a lower incidence in children. The team of Sun Jie, director of the Shanghai Children's Medical Center affiliated to the National Children's Medical Center & Shanghai Jiao Tong University School of Medicine, summarized the rich experience accumulated in the diagnosis and treatment of children's pheochromocytoma diseases over the years, and with the support of related disciplines such as anesthesia, accumulated valuable experience in safely completing the whole process management and surgical treatment of pediatric pheochromocytoma, and formed the surgical approach characteristics and operation skills of their own team. After selection, today we bring you a typical case of pediatric pheochromocytoma patients treated with posterior laparoscopic surgery for sharing for your reference and learning!
<h1 class="pgc-h-center-line" data-track="6" > case introduction</h1>
General information: Male, 8 years old.
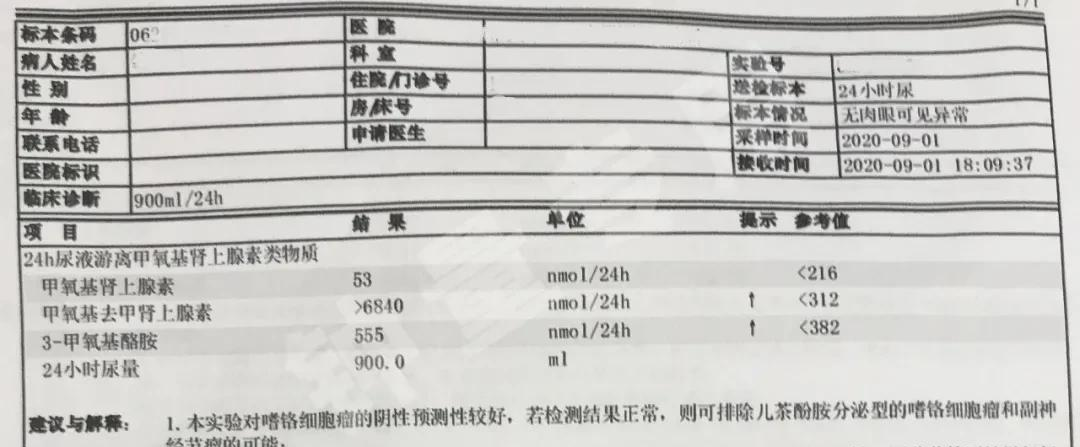
Current medical history: Admission to hospital for half a month due to recurrent headaches. Admission suggests blood pressure of 138/101 mmHg, abdominal CT suggests a right adrenal tumor, and pheochromocytoma may be. 24-hour urine free methoxyephrine-like examination suggests: methoxy norepinephrine 6840nmol/24H (normal value less than 312nmol/24H), methoxyephrine 53nmol/24H (normal value less than 216nmol/24H), 3-methoxytylamine 555nmol/24H (normal value less than 382nmol/24H). Specific markers of PPGLs: 3-Methoxytyramine 0.27 nmol/L (normal value less than 0.18 nmol/L), methoxyephrine 0.11 nmol/L (normal value less than or equal to 0.18 nmol/L), methoxy norepinephrine greater than 20.56 nmol/L (normal value less than or equal to 0.90 nmol/L).
preoperative examination:
Urine test
Specific marker testing for PPGLs

Preoperative CT imaging
Preoperative MRI images
Surgical position and torcar distribution indications:
<h1 class="pgc-h-center-line" data-track="60" > preoperative preparation and surgical treatment</h1>
Preoperative preparations are given 5 mg b.i.d. orally with infusion and volume expansion. After three days of taking the drug, the patient complained of nasal congestion and occasional nosebleeds. This dose was maintained orally, and post-laparoscopic right adrenal tumor resection was performed after two weeks of expansion.
Intraoperative free tumor body blood pressure up to 180/110 mmHg, nicardipine is given to lower blood pressure to normal and continue to be free. After a complete free tumor, blood pressure drops to 80/30 mmHg, nicardipine is discontinued immediately, and blood pressure returns to normal levels.
Postoperative return to the general ward for ECG monitoring, routine rehydration, no use of vasoactive drugs and antihypertensive drugs. Within two days of postoperative ECG monitoring, blood pressure fluctuated around 100/60 mmHg and heart rate fluctuated at around 120 bpm. The patient had no discomfort except for the main complaint of palpitations. After that, it was observed until five days after the operation, and the palpitation symptoms gradually disappeared.
Surgical specimens:
Postoperative follow-up: two weeks after discharge, blood pressure and heart rate were normal, 24-hour urine methoxy norepinephrine 115nmol/24H (normal value is less than 312nmol/24H).
<h1 class="pgc-h-center-line" data-track="61" > expert reviews</h1>
Professor Sun, hello, from the operation video, affected by the smaller surgical area of pediatric patients than adults, the interval between our several channels is relatively close, and the convergence of the direction of the operating instruments can be seen from the intraoperative perspective is very strong, so why do most of our team choose to complete this operation through the posterior abdominal cavity?
Hello, there are two main reasons. Although according to our traditional view, the posterior abdominal space in children is relatively small. But correspondingly, there is also less extraperitoneal fat and perirenal fat in children. Therefore, after the retroperitoneal space is established, there is no need for further free fat. In fact, it is more convenient to operate, not as small as imagined and inconvenient to operate. Second, compared with the anterior abdominal approach, the posterior abdominal approach can reach the kidneys and adrenal glands, without the need for additional auxiliary channels to push away the intestine and liver and spleen, further reducing trauma, enhancing the confidence of patients and parents, and alleviating their anxiety.
What are the special features of preoperative expansion medication for pediatric patients?
Preoperative expansion in children still requires the dose of phenopene according to kilogram body weight, and the initial dose in children is 0.2 mg/kg (the total dose < 10 mg) 4 times a day, in increments of 0.2 mg/kg. Increase the intake of salty fluids in the diet during medication to reduce the occurrence of orthostatic hypotension and help to expand capacity. And it needs to be adjusted in time according to the child's response, generally speaking, the preparation time will take 2 weeks, and the child's nasal congestion and limb warmth are appropriate indicators of expansion.
<h1 class="pgc-h-center-line" data-track="62" > expert introduction</h1>
Prof. Jie Sun, Chief Physician, Deputy Director of the Department of Major Surgery of the National Children's Medical Center and Shanghai Children's Medical Center, Director of The Department of Urology, Doctoral Supervisor
Dr. Zhong Liang, Attending Physician of Urological Stones Specialty Group of National Children's Medical Center & Shanghai Children's Medical Center