The affected child, 6 years old, coughed for 2 weeks, did not have fever, aggravated 2 days of outpatient visits, blood test indicators are as follows:
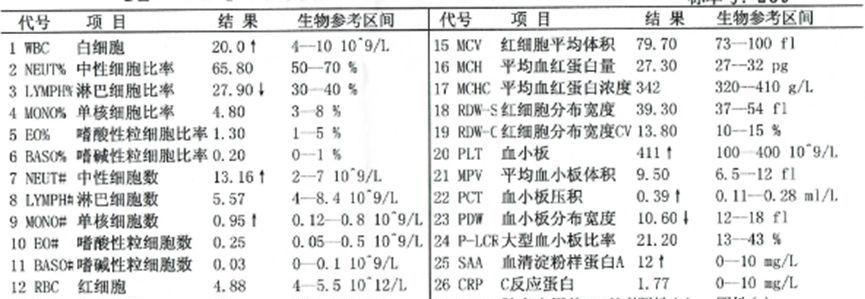
Leukocytes 20×109/L (elevated), neutrophil ratio 65.8% (normal), neutrophil number 13.16×109/L (elevated), C-reactive protein 1.77 mg/L (normal).
White blood cells are high, but C-reactive protein is normal, so what is the relationship between white blood cells and C-reactive protein? Is it the basis for the use of antibiotics?
Understanding the clinical significance of C-reactive proteins and white blood cells, as well as the relationship between them, is very helpful for our clinic.
C-reactive protein (CRP)
CRP is a capable of binding to streptococcus pneumoniae capable of capable of capable C polysaccharides, formed by 5 identical subunits (23KD) in non-covalent bonds to form a cyclic pentamer protein with a molecular weight of 115KD and a half-life of 19h, mostly stimulated by inflammatory molecules such as interleukin-6 (IL-6) to stimulate liver cell synthesis. The serum content of CRP in normal people is very small.
CRP is a protein that rises sharply in the blood plasma when the body is infected or the tissues are damaged. CRP usually begins to rise 6 to 8 hours after the initial onset of the disease and peaks at 24 to 48 hours, and the magnitude of the increase is positively correlated with the severity of infection or inflammation. Normal CRP range: < 10 mg/L.
Viral infection
Serum CRP levels are often normal or mildly elevated.
Bacterial infections
When bacterial infection, 88% to 94% of patients have CRPs in excess of 50 mg/L, and 80% of patients have CRPs in excess of 100 mg/L. Focal or superficial infection is often suggested when the CRP level is 10 to 99 mg/L, and sepsis or invasive infection is more common when the ≥ 100 mg/L. During anti-infective therapy, dynamic monitoring of changes in CRP levels can help determine efficacy, and a decrease in CRP to normal can be used as one of the indicators of discontinuation.
shortcoming
Although CRP is more specific than changes in white blood cell count, it is not highly specific and can be significantly elevated in many noninfectious diseases such as trauma, surgery, myocardial infarction, malignancies, and especially autoimmune diseases.
Clinical significance of white blood cells (WBCs).
WBC is a class of cells with phagocytic function and are an important part of the body's immune defense system. When an infection occurs, the largest number of neutrophils in white blood cells increases rapidly (manifested by an increase in the number of white blood cells), engulfing pathogens such as bacteria and parasites that invade the body.
And the increased number of white blood cells is often proportional to the degree of bacterial infection. However, when the virus invades the body, white blood cells tend not to rise, or rise slightly.
In addition, various tissue injuries, trauma, postoperative, acute blood loss, poisoning, malignant tumors, acute poisoning and other conditions of white blood cells will also be significantly increased, but this should be judged and analyzed according to the patient's situation and other examination methods.
Clinical significance of WBC and CRP

WBC and CRP are interrelated
Elevated white blood cells may indicate infection, but they are insensitive in localized infections and aseptic inflammation. In patients with leukopenia and infection, the white blood cell count is of no value, and there are many factors that affect the elevation of white blood cells, such as intense physical activity.
CRP is an acute phase reactive protein, and tissue damage is related to the degree of infection, the most obvious increase in severe infection caused by gram-negative bacteria, the mildest increase in CRP caused by viral infection, but other inflammation and tissue damage can also cause CRP elevation, which needs to be considered comprehensively.
WBC is slightly elevated, CRP is not elevated.
Influencing factors
WBC is susceptible to factors such as age, daytime changes, pregnancy and childbirth, and medication, while CRP is not affected by physiology, immune status, and medication.
In normal people, due to the physiological changes of WBC, especially the white blood cells of young children, the white blood cells are greater than 10×109/L, and the CRP is negative, which is within the healthy range.
The elderly have poor response to the disease, the total number of white blood cells cannot increase accordingly after infection, and the CRP is positive beyond the normal range, which can assist in clinical diagnosis.
WBC foundation level
Some patients originally had a low leukocyte base, usually (4-5) × 109/L, rising to 10×109/L when infected, which is still in the normal range, while CRP is elevated beyond the normal range (positive), which helps to diagnose.
Speed of reaction at the time of infection
WBC rises more slowly and changes slowly after treatment, while CRP changes more rapidly, can be seen for a few hours, and returns to normal within 1 week with cure.
Activity of the associated disease
Changes in the amount of WBC do not reflect disease activity; dynamic changes in CRP volume can reflect disease activity. The use of the drug can be adjusted according to changes.
analyse
The child's white blood cells and neutrophils are high, but the percentage of neutrals is not high, and the inquiry learned that the dance rehearsal was more than 1 hour on the day and the intensity was large, which may be the reason for the high level of these two indicators, because high and mild exercise will cause white blood cells to exceed the normal range.
Based on the examination results and clinical symptoms, the diagnosis is upper respiratory tract infection, symptomatic treatment of cough, no anti-infective treatment, and the following tests are repeated after 3 days:
In summary, the inconsistencies between WBC and CRP should be combined with clinical comprehensive consideration and the causes analyzed.
The two play a synergistic diagnostic role in the diagnosis of bacterial infectious diseases, but CRP is more sensitive than WBC, and is a clear and sensitive indicator of inflammation and tissue damage in diagnosis, prognosis, efficacy observation, and partial screening.
【Reference】
Infectious Diseases Committee of China Medical Education Association. Expert consensus on the interpretation of the clinical significance of infection-related biomarkers[J]. Chinese Journal of Tuberculosis and Respiratory Disease, 2017, 40(4):243-257.
Source: Clinical Pharmacy Channel of the Medical Community
Edited by: Yeah Reviewer: Xiao Ran