Upright, exhaled, and lateral chest x-ray are the best way to confirm pneumothorax, but sometimes due to the patient's condition, only supine x-rays can be used, which can make pneumothorax diagnosis difficult. Deep groove may be the only pneumothorax sign in the supine position. Patients with traumatic pneumothorax can only be examined in a flat position because of the need to protect the cervical spine, in which case the sensitivity of the X-ray examination will be greatly reduced, and it has been reported that it can be reduced to 36% to 48%. In recent years, bedside ultrasound has played an important role in the diagnosis of such patients and should be taken seriously.
Case 1
Patient age: 40 years
Patient sex: Female
After a road traffic accident, he was taken to the emergency room. Upon arrival, the patient was conscious, hemodynamically stable, with a respiratory rate of 14 breaths per minute, a pulse rate of 81 beats per minute, and a blood pressure of 141/86 mmHg.
Physical examination reveals multiple limb injuries in addition to tenderness in the right chest wall on palpation.
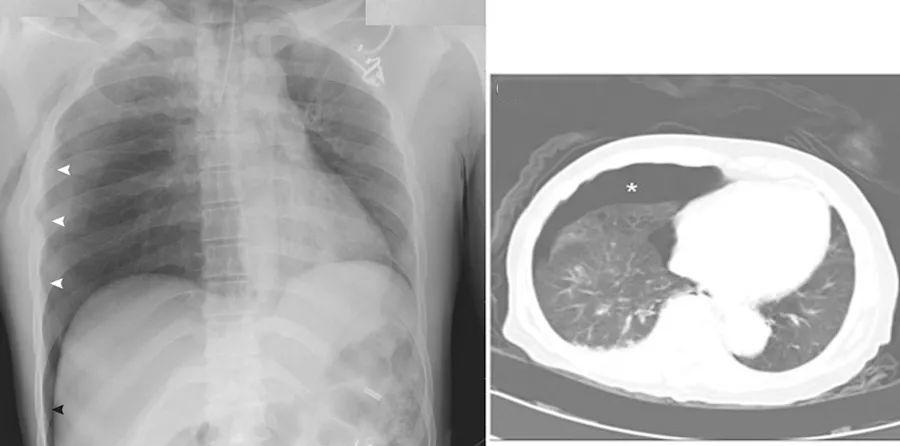
Supine chest x-ray shows a limited increase in luminosity of the pneumothorax (white arrow) and right rib angle, which may appear as a sharply edged translucent area pointing to the quarter rib (black arrow).
Chest CT confirms pneumothorax (asterisk) and atelectasis.
A closed chest drain is placed and repeated chest x-rays show right lung brachial reassurance.
Case 2
Age of patients: 56 years
Patient sex: Male
The builder, hit by a falling metal beam, suffered severe blunt injuries to his head, chest and lower limbs. Emergency examination, confusion, blood pressure of 111/59 mmHg, pulse rate of 103 beats / min, respiratory rate of 28 breathing rate / min, dyspnea.
Ultrasonography shows a bar code mark above the left chest. After chest x-ray, the respiratory rate increases to 36 breaths/min. Emergency left pneumothorax closed drainage, improved breathing. Post-perfected CT (coronal surface) of the chest suggests pneumothorax, lung atrophy, and deepening of the ribic diaphragm angles.
Clinical diagnosis: rib fracture; pneumothorax

The patient is in stable condition and is transferred to a higher hospital.
Past notes
Spontaneous pneumothorax with a family history
Histiocytosis secondary to lung Langerhans cell histiocytosis
2022-01-18