Thanks to the Lilac Garden Station friends @ Small City View for sharing the case ~
Patient: Male, 55 years of age.
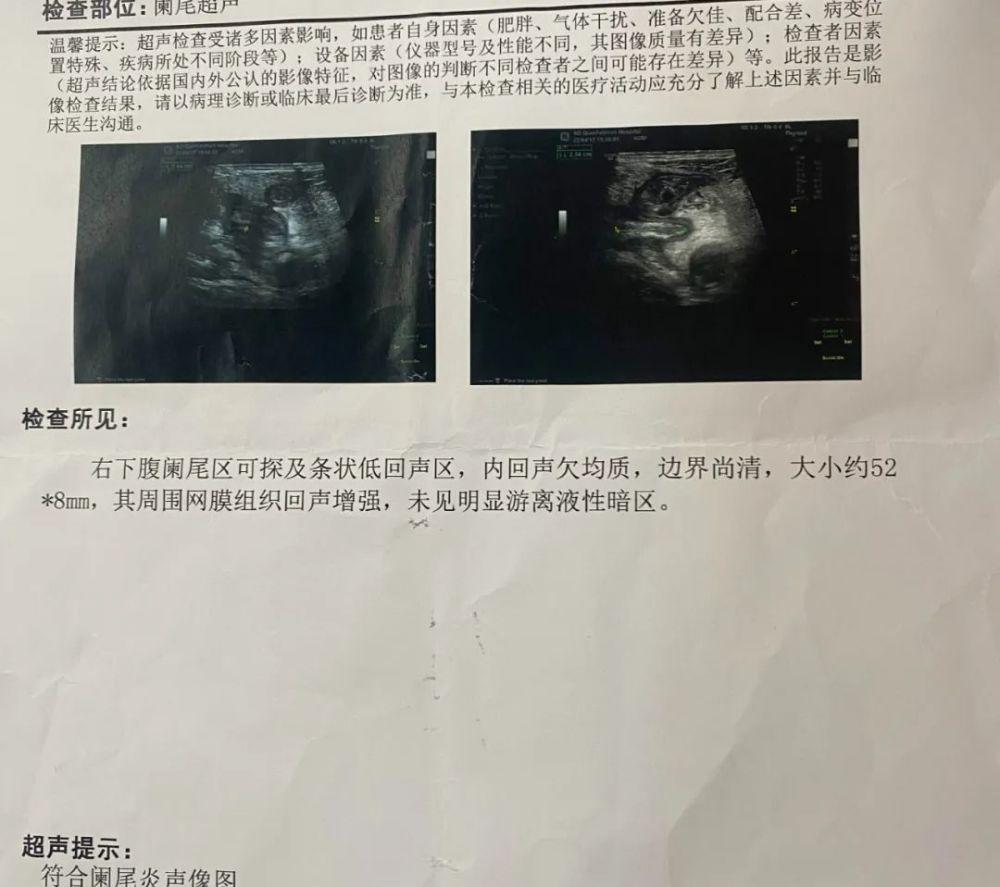
Brief medical history: metastatic right lower quadrant pain 2 days admission, no fever outside the hospital, no nausea, vomiting, no discomfort such as melena. Outpatient ultrasound prompt: acute appendicitis sonogram, so as to receive acute appendicitis. Patients deny a prior history of the disease. Denial of history of alcohol and tobacco.
Physical examination: flat abdomen, no rash and abnormal varicose veins in the abdominal wall, no gastrointestinal type, full abdominal softness, no mass touched, no fluid wave tremor, tenderness in the right lower quadrant, no obvious rebound pain. Full-abdomen drumming, mobile voiced negative. Bowel sounds 4 times per minute, no abnormal vascular murmurs are heard.
Adjunctive tests: outpatient ultrasound:
Admission blood test (no tumor marker program)

CT after admission :
Clinical diagnosis: acute appendicitis
Treatment: Hydration after admission, anti-infection treatment. After the results of the examination were presented, laparoscopic appendectomy was performed, and the posterior ileal appendix was seen during the operation, adhesion to the surrounding intestinal duct, covered with pus, and after separation, the appendix was significantly swollen, the wall was thick, and the size of the appendix was about 6 × 0.5 cm. The ileo blind part is dissected clearly, and the appendix is cut from the root of the appendix after the appendix artery is cut off. Consider the thickness of the appendix wall, intraoperative rapid pathology, pathological feedback: consistent with acute purulent appendicitis. Rinse and place drainage after suturing the incision.
Intraoperative rapid:
Continue to rehydrate after surgery to fight infection. The patient has no postoperative fever, drainage is unimpeded, and approximately 200 ml of reddish liquid is drained. The test indicators of postoperative review are as follows:
Postoperative pathology
If this patient is your primary treatment, what should you do next?