*For medical professionals only
Propranolol can also be used in this way!
β-blockers (β-B) are probably familiar to everyone, and because of their age and pharmacological properties, they are often classified into three generations:
■ The first generation is non-selective β-B;
■ The second generation is a selective beta1 blocker, and the first and second generations are often referred to as "traditional β-B";
■ The third generation is β-B with vasodilatory effect: including α/β blockers that exert vasodilators by blocking α1 receptors, and new generation β-B (such as nibivolol, etc.) that do not block through α1 receptors but have endothelial-dependent vasodilation effects.
Among them, propranolol is a fat-soluble non-selective β-B[1], which is often used clinically for the treatment of hypertension, coronary heart disease, arrhythmias, cardiomyopathy, pheochromocytoma and other diseases, but due to the non-selectivity of propranolol, in recent years, many guidelines in the cardiovascular field have downgraded the status of propranolol in clinical treatment to varying degrees.
So, is propranolol really "OUT" in clinical applications?
Answer: Not really!
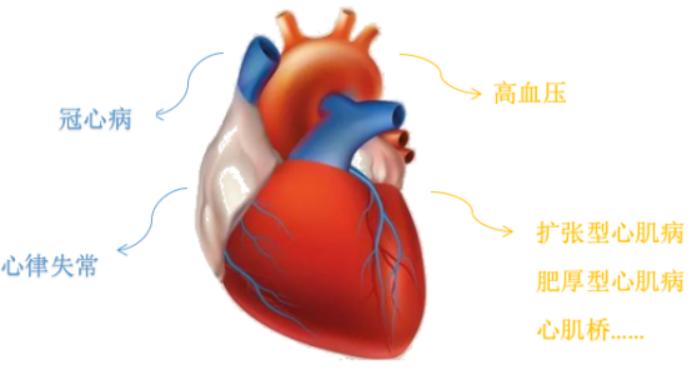
Fig. 1 Cardiovascular indications for propranolol (Source: self-made)
Although the major guidelines for cardiovascular diseases for propranolol is not high recommended level, but propranolol is still the first-line choice for the treatment of other diseases, and then the small medicine will take everyone to know the extracardiac clinical application of propranolol, an "old drug".
One
Hyperthyroidism
Hyperthyroidism (hyperthyroidism) refers to an endocrine disorder caused by the improper and continuous synthesis and secretion of too many thyroid hormones by thyroid glands. Toxic diffuse goiter (Graves disease) is the most common type of hyperthyroidism, and is more prevalent in women than in men.
Excessive secretion of thyroid hormones will cause a series of clinical symptoms, will improve the excitability of the cardiovascular nervous system, resulting in respiratory, heart rate acceleration, increased thermogenesis, patients can feel palpitations, shortness of breath, activity can be further aggravated, severe cases can occur myocardial ischemia, heart enlargement, heart failure and so on.
Propranol inhibits the elevation of catechol ammonia by acting on β-receptors, blocking the activity of β-receptors of the target organ, and improving symptoms such as irritability, heat intolerance, hyperhidrosis, tachycardia, and muscle tremor in patients [2].

Figure 2 Thyroid diagram (Source: made by yourself)
In addition, non-selective β-B can also inhibit the conversion of peripheral tissue thyroxine (T4) to triiodothyronine (T3), blocking the direct effect of thyroid hormones on the myocardium, but because it also blocks the secretion of parathyroid hormone, it is necessary to pay attention to the regulatory effects of calcium and phosphorus in patients.
Table 1 Distribution of β1 and β2 receptor thyroid and parathyroid glands and their mediated physiological roles[3]
The "Guidelines for the Primary Diagnosis and Treatment of Hyperthyroidism (2019)" recommends that β-B be used in the elderly, patients with a resting heart rate> of 90 beats/min or concomitant cardiovascular disease, preferably β1 and β2 receptor blocker propranolol hydrochloride, administered at a dose of 10 to 40 mg/day, orally every 6 to 8 hours, and if the patient has bronchial asthma or wheezing bronchitis, selective β1 receptor blockers such as metoprolol can be used.
Therefore, propranolol is the preferred agent when β-B is required in patients with hyperthyroidism.
Two
Infantile hemangiomas
Hemangioma, also known as infantile heman-gioma (IH), is the most common benign vascular tumor in infants and young children, with an incidence of about 1% to 12%, and it is increasing year by year.
It is characterized by endothelial cell proliferation and neovascularization, which begins to resolve spontaneously around the age of 1 year, and generally resolves at the age of 5 to 10 years. Although IH occurs in all races, the incidence is higher in Caucasians and is higher in girls than in boys [4-5].
IH is a benign tumor, although some of it can resolve spontaneously, but because IH often occurs in infants and young children in the head and neck position, it will bring serious psychological burden to children and parents, so except for IH that grows in a hidden area, is small in size, and is in a stable state can be observed and treated first, and other cases require active treatment [6].
With the release of a large number of clinical research results, oral propranolol has gradually become a first-line drug to replace glucocorticoids for the treatment of IH [7], and its mechanism of action is numerous, including immediate effect, medium effect mechanism, long-term mechanism, etc., with the immediate effect more obvious and rapid.
Figure 3 Children with IH (Source Network, if there is infringement, please contact to delete)
Table 2 Mechanism of action of propranolol in the treatment of IH[5]
There have also been studies showing that yellow people are more sensitive to propranolol in the treatment of IH [8].
Therefore, domestic experts have formed an expert consensus specifically for the treatment of propranolol for IH, that is, the "Chinese Expert Consensus on oral propranolol for the treatment of infantile hemangioma", which involves indications and contraindications, pre-treatment examination, medication methods, etc.
Three
Prevention of bleeding from esophageal gastric varices
Esophageal gastric varices (GOV), one of the clinical manifestations of portal hypertension, and in severe cases, esophageal gastric varices rupture bleeding (EVB) is one of the most common digestive emergencies [9].
Fig. 4 Schematic diagram of esophageal gastric varices
(Image source network, if there is infringement, please contact to delete)
Nonselective β-B, such as propranolol, reduce cardiac output by blocking the heart's beta1 receptors, blocking the β2 receptor reflex of visceral blood vessels, constricting visceral arteries, reducing portal hypertension, and preventing varicose vein rupture and bleeding [10].
In fact, for patients with portal hypertension in cirrhosis, there is some controversy about whether to use non-selective β-B as a primary prevention of EVB and the prevention and treatment of mild esophageal gastric varices.
However, in the Guidelines for the Prevention and Treatment of Portal Hypertension and Gastric Variceal Bleeding in Cirrhosis, it is recommended that non-selective β-B or endoscopic (EVL) be used to prevent first varicose bleeding in patients with moderate or severe esophageal gastric varices and a greater risk of bleeding (A,1).
Nonselective β-B is preferred for those at low risk of bleeding, and EVL (B, 2) is preferred for those with contraindications to nonselective β-B, intolerance, or poor adherence.
Guidelines also mention that propranolol starts at 10 mg bid and can be gradually increased to the maximum tolerated dose, and carvedilol starts at 6.25 mg, qd, and can be gradually increased to the maximum tolerated dose if tolerated. Therefore, non-selective β-B in patients with GOV can be used after assessing the overall condition of the patient and deciding whether to use it.
What other drugs do you want to know about their clinical use? Come and let us know in the comments section!
bibliography:
[1] Α/β the chinese expert consensus on the application of receptor blockers in the treatment of hypertension.
[2] Guidelines for primary diagnosis and treatment of hyperthyroidism (2019).
[3] β expert consensus on the use of adrenergic blockers in cardiovascular disease.
[4] Phung TL, Hochman M. Pathogenesis of infantile hemangioma[J]. Facial Plast Surg, 2012, 28(6): 554-562.
[5] Song Huixin,Lin Chunnan,Wang Tianyou,Fu Zhaochen. Research progress on the mechanism of action of propranolol in the treatment of infantile hemangiomas[J]. Chinese Journal of Oral and Maxillofacial Surgery,2020,02:182-185.]
[6] Zheng Jiawei, Wang Xukai, Qin Zhongping, Fan Xindong, Li Kai, Yang Yaowu, Huo Ran, Liu Shaohua, Zhao Jihong, Wang Xiaoyong, Zhou Dekai. Chinese expert consensus on oral propranolol in the treatment of infantile hemangioma[J]. Shanghai Journal of Stomatology,2016,03:257-260.
[7] Léauté -Labrèze C, Dumas de la Roque E, Hubiche T, et al. Propranolol for Severe Hemangiomas of Infancy [J]. N Engl J Med, 2008,358(24):2649-2651.
[8] Zhou HH, Koshakji RP, Silberstein DJ, et al. Altered sensitivity to and clearance of propranolol in men of Chinese descent as compared with American whites [J]. N Engl J Med, 1989,320(9):565-570.
[9] Xu Xiaoyuan, Ding Huiguo, Jia Jidong, Wei Lai, Duan Zhongping, Ling Hu Enqiang, Liu Yulan, Zhuang Hui, Cao Ying, Fu Fu chuan, Zhang Yan, Zhang Xiaxia. Guidelines for the prevention and treatment of portal hypertension of gastrointestinal variceal bleeding[J].Practical Journal of Liver Disease,2016,19(05):641-656.
Jiang Meichun,Wang Anjiang,Zhu Xuan. The use and controversy of non-selective β receptor blockers in cirrhosis and esophageal gastric variceal veins[J].Chinese Journal of Practical Internal Medicine,2018,38(12):1144-1148.
More good articles on clinical medication
Follow the Clinical Pharmacy Channel to view
Source: Clinical Pharmacy Channel of the Medical Community
Author: Ran Sasha
Editor-in-charge: Zheng Huaju
Proofreader: Zang Hengjia
Plate making: Xue Jiao