Legionella pneumonia, how much do you know?
Legionella is a "killer" lurking around us, some of its symptoms are similar to new crown pneumonia, and it is easy to develop severe disease, with a case fatality rate of 5% to 30% [1]. After Legionella invades the human body, the attack is fierce, and it can lead to the death of patients within 7 days, most of the patients die because of respiratory failure, followed by shock and acute renal failure.
1
Origin of Legionella
Legionella, also known as "Legionella veterans," first broke out in 1976 during the Annual Meeting of Veterans in Philadelphia, USA, where 221 people fell ill and 34 died, isolating pathogens from autopsy organizations and naming them Legionella. There are currently 52 species, 3 subpopulations, 70 serotypes known for Legionella, and 24 species associated with human diseases, the most common of which is Legionella pneumophila, which mainly causes Legionella pneumonia [2].
Legionella breeds at 25 °C to 43 °C, the most suitable growth temperature is 35 °C, and the incidence of Legionella pneumonia is higher in July, August and September every year. Legionella likes to survive and spread in warm water and hot flashes, and air conditioners, water heaters, showers, hot springs, etc. are all hotbeds for its growth and reproduction.
Therefore, before turning on the air conditioner in the summer, it is recommended to properly clean and disinfect the air conditioner. Prevention of Legionella can choose disinfection interventions according to different situations: (1) copper and silver ions (2) heating to 60 ~ 77 ° C and rinsing (3) ultraviolet radiation to local areas.
2
Pathogenic mechanism
The pathogenic mechanism of Legionella is mainly in two aspects: one is the intracellular life cycle, and the other is the virulence island genome and virulence gene of bacteria [1].
1. Intracellular life cycle: Legionella invades human macrophages through the adhesins and infectins of bacteria, multiplies intracellularly, and forms phagosomes, toxins and virulence factors.
2. Virulence Island Genome and Virulence Gene: According to nucleotide sequence analysis, there is a Virulence Island with a relative molecular mass of 65,000 in the 80,000 bp gene region of Legionella pneumophila. These virulence genes play an important role in bacteria invading host cells, killing human macrophages and multiplying within cells, and are important factors in the pathogenesis of Legionella pneumophila.
3
When to consider Legionella pneumonia
Legionella is transmitted in a similar way to the new coronavirus, where the human body becomes sick from inhaling an aerosol infection containing Legionella! The bacteria invade the body from the respiratory tract, causing pneumonia, pleurisy, vomiting, diarrhea, and even shock and death. Moreover, Legionella pneumonia specializes in picking up "soft persimmon pinches", and people with low immunity, such as the elderly, children, pregnant women, and patients with underlying diseases, are often the objects of his attention. According to the WUH scoring system [2], if the above populations: (1) body temperature > 38.9 °C (with relative bradycardia) ;(2) erythrocyte sedimentation rate > 90 mm/h or C-reactive protein > 180 mg/L; (3) ferritin is 2 times higher than normal; (4) hypophosphatemia; (5) phosphokinase is > 2 times higher; (6) microscopic hematuria at admission. If there are more than 3 of these and there is no response to β-lactam antimicrobials, Legionella pneumonia is highly suspected.
Or, according to the Guidelines for the Diagnosis and Treatment of Adult Community-Acquired Pneumonia in Adults (2016 Edition), the possibility of Legionella pneumonia should be considered when adult CAP patients have fever with relative bradycardia, acute onset headache, non-drug-induced confusion or drowsiness, non-drug-induced diarrhea, shock, acute liver and kidney function injury, hyponatremia, hypophosphatemia, and no response to β-lactam antibacterial drugs.
4
Diagnosis of Legionella[1]
(1) Positive Legionella culture is the gold standard for diagnosing Legionella infection, but the positive rate is low, and the use of early anti-sensing drugs may cause false negatives, and the use of bronchoalveolar lavage (BALF) and lung biopsy specimens can improve the positive rate.
(2) Legionella pneumobacterium type 1 urinary antigen detection can be used for early rapid diagnosis, and the results are not affected by early anti-infective therapy.
(3) Although the detection of Legionella antigens in qualified lower respiratory tract specimens has the advantages of rapid, simple, can be identified by genus species, and can distinguish subtypes, it is sensitive and specific.
5
Image features
The relative specificity of the chest image of Legionella pneumonia is that the ground glass shadow is mixed with a solid variable with relatively clear edges. Imaging progression over a short period of time (within 1 week), or full absorption of pulmonary infiltrates after weeks or even months is also characteristic of Legionella pneumonia despite improvement in clinical symptoms [3].
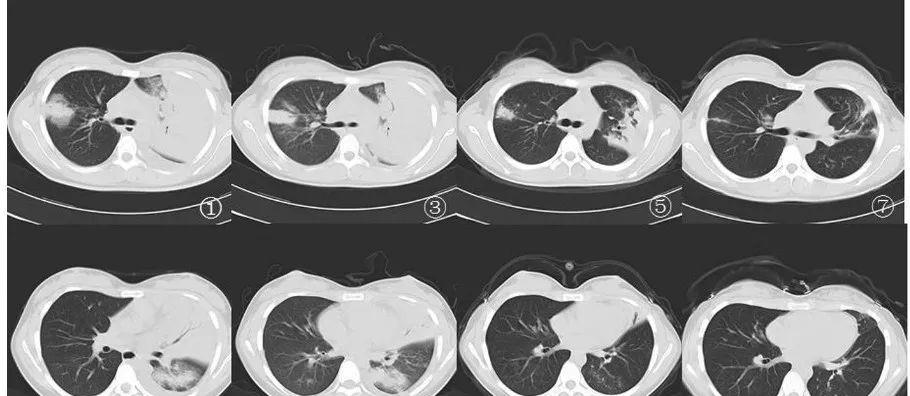
Figure 1-
Note: On the first day of admission, chest CT showed multiple patchy exudation of both lungs, solid changes in the left upper lung, bronchial inflatable signs were visible inside, accompanied by a small amount of pleural effusion on the left side; after one week of treatment, the right upper lobe exudation was slightly reduced, and the left pleural effusion was reduced (after chest puncture); after 6 weeks of treatment, the absorption of both lung exudates was significantly improved; the two lung exudation shadows were basically absorbed, and the cavities formed after the discharge of fibrous cords and necrotic substances in the upper left lung lobe [4].
6
treat
Legionella is an endocytotic parasitic bacterium that invades macrophages through the respiratory tract and then invades macrophages for growth and reproduction. Therefore, anti-infective drugs that are effective against Legionella depend on anti-Legionella activity and its concentration in alveolar macrophages. β lactams and aminoglycosides have a poor effect on the treatment of Legionella pneumonia because they cannot penetrate cell membranes. Commonly used drugs currently available for the treatment of Legionella infections include quinolones, macrolides, and doxycycline, while tigecycline, co-trimoxazole, and rifampicin have also been shown to be effective against Legionella infections.
Patients with mild and moderate Legionella pneumonia with normal immune function may be treated with macrolides, respiratory quinolones, or doxycycline monotherapy, and for severe cases, failure of monotherapy, and immunocompromised patients, treatment with quinolones plus rifampicin or macrolides is recommended. When quinolones are treated with macrolides, the potential risk of developing cardiac electrophysiological abnormalities should be alerted.
Specific usage [5]: Levofloxacin 750 mg orally/intravenously once daily for 7 to 10 days is preferred, moxifloxacin 400 mg orally/intravenously once daily for 7 to 10 days, or azithromycin 500 mg orally/intravenously once daily for 7 to 10 days. Rifampicin 300 mg orally/intravenously twice daily (not mandatory), in combination with other listed drugs.
Alternative: Erythromycin 1 g / 6 h intravenously, followed by 500 mg orally 4 times a day for 7-10 days. Ciprofloxacin 400 mg every 12 hours, intravenously, then 750 mg each time, orally 2 times a day for a total of 7-10 days.
Other sites of infection: endocarditis: fluoroquinolones (same as the above pneumonia) + rifampicin 300 mg orally twice daily for 4-6 weeks, usually requiring valve replacement.
bibliography:
Respiratory Diseases Branch of Chinese Medical Association. Chinese Guidelines for the Diagnosis and Treatment of Adult Community-Acquired Pneumonia (2016 Edition)[J].Chinese Journal of Tuberculosis and Respiratory Diseases,2016,39(4):253-279.DOI:10.3760/cma.j.issn.1001-0939.2016.04.005.
Liang Sicong,Chen Yu. Diagnosis and treatment strategies of Legionella pneumonia[J].Chinese Journal of Practical Internal Medicine,2020,40(5):357-361.
Pang Li,Zhang Duchao,Qin Chong,Liu Jia,Pan Lei. Clinical analysis of 39 cases of community-acquired Legionella pneumonia[J].Labeled Immunoassays and Clinical,2021,28(5):748-752.
Shang Yuejing. Imaging manifestations and diagnostic value of community-acquired Legionella pneumonia[J].Primary Medical Forum,2011,15(28):938-940.
[5] John. Hopkins, ABX Guide.p334-335.
This article was first published: Respiratory Channel of the Medical Profession
【Copyright Notice】This platform is a public welfare learning platform, reprinted for the purpose of transmitting more learning information, and has indicated the author and source, such as teachers who do not want to be disseminated can contact us to delete
![About drug-resistant tuberculosis[fig]](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACwAAAAAAQABAAACAkQBADs=)