At present, the domestic valves on the market are self-expanding valves, the corolla part of the valve frame is located in the ascending aorta, and the catheter is difficult to put in place the coronary artery opening due to the interference of the valve frame body, so it is more difficult to intervene in the coronary artery again after TAVR.
A new domestic SinoCrown valve (Lepu Medical, Beijing) is designed for the short valve frame but released in a self-expanding manner, which is convenient for coronary artery intervention in patients after TAVR surgery.
SinoCrown valves have obvious structural differences with the previously listed domestic self-expanding valves and foreign balloon dilated valves, and their advantages include:
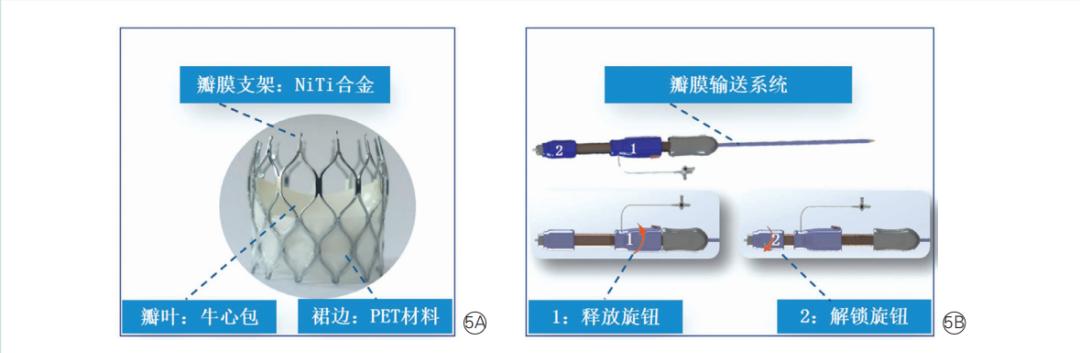
(1) Frame characteristics: short stent with very little insertion, unique inner and outer skirt can reduce perivalvular leakage, excellent hemodynamic characteristics, excellent support and adapt to patients with bifoliary aortic valve, with positioning marks.
(2) Leaflet characteristics: Bovine pericardial leaflet leaf is durable.
(3) Release features: full hanging head connection, combined with a fully recyclable repositioning conveyor system, can achieve 100% complete recovery; unique release process, the development is extremely stable;
(4) The most distinctive design concept: the release process is in the form of a long valve, the stability of the valve insertion process is enhanced, and it does not bounce; after unlocking, the short valve form is placed in the body, and the risk of obscuring the coronary artery orifice is low, which is convenient for the coronary artery to intervene again in the later stage (Figure 5).
This case is the first time that the SinoCrown valve has been applied to a patient under clinical study. This is a patient with severe aortic valve calcific stenosis who had a left anterior descending stent inserted in the outer courtyard 7 years ago due to chest tightness.
Aortic root anatomy was evaluated with 3Mensio software: the aortic valve was functional bilobasic valve, the left and right lobe lobes were calcified at fusion, and the valve lobe calcification was heavy (total calcified volume 1579.0 m3); the coronary artery opening height was acceptable (left: 19.7 mm, right: 18.5 mm); the length and shortness of the valve ring were 23.8 mm×29.8 mm, the circumference was 85.8 mm, and the area was 569.0 mm2.
Other CT measurement parameters are detailed in Figure 1, and the multiplane measurement parameters on the valve and the full aortic assessment are shown in Figure 2.

Despite an STS score of 1.288%, it is a low risk of surgery, and patients refuse surgery. The aortic valve was anatomically appropriate for TAVR; the life expectancy after correction of severe aortic stenosis was more than 1 year, in line with the TAVR indications, and there were no surgical contraindications, so IT was decided to perform TAVR.
Ultrasound-guided precision puncture of the right common femoral artery as the main approach and puncture of the left common femoral artery as a secondary approach; two ProGlides are embedded in the right common femoral artery, guided by a lunderquiest superhard steel wire, placed in a 22 F DrySeal sheath tube, and immediately given heparin 5,000 units of heparin for systemic arterial heparinization; temporary pace electrode implanted at the right ventricular apex through the right femoral vein.
Advance coronary angiography shows 80% proximal stenosis of the stent of the left anterior descending branch, pre-dilation with a 2.5 mm × 15.0 mm Maverick balloon followed by a 2.75 mm × 18.00 mm GuReater stent.
Aortic root angiography was performed using the right sinus center projection position (3°left, head 11°), the AL2 catheter was used with the straight-headed ultra-slipper loach guide wire for cross-flap, and then exchanged for a plastic lunderquiest superhard steel wire at the end of the head, and the narrow calcified aortic valve was pre-expanded with a 25.0 mm × 40.0 mm NUMED-II balloon, and the aortic root showed no peri balloon leakage and coronary artery blood flow.
The 27-type SinoCrown valve was selected according to the preoperative plan, and the valve delivery system smoothly passed through the aortic arch and across the aortic valve, and the SinoCrown valve was positioned according to the calcification of the valve leaf and the angle of the no-crowned sinus floor.
The right ventricle rapid pacing was used 180 beats/min to reduce the patient's systolic blood pressure below 50 mmHg, at which point the SinoCrown valve began to be slowly released, and the rapid pace was stopped immediately when the newly inserted valve was in working condition; at this time, the aortic root angiography showed that the SinoCrown valve was in an ideal position, with a small amount of perivalle leakage; at the same time, the SinoCrown valve position and valve frame were well unfolded by esophageal echocardiography, only the micro perivalular leakage, the peak flow rate and the transvalvular pressure difference were within the normal range.
After rotating the unlock knob, the valve delivery system and the SinoCrown valve are gradually separated, only the SinoCrown valve is placed in the aortic valve position, followed by angiography showing successful Insertion of the SinoCrown valve, no valve displacement and significant perivalular leakage (Figure 3); the esophageal echocardiogram reconfirms the SinoCrown valve position and morphology, the trace perivalle leakage, the peak flow rate of 1.7 m/s and the cross-valve pressure difference is 7 mmHg, and the left ventricular ejection fraction is 60%.
After successful TAVR treatment, the patient was transferred back to the intensive care unit of internal medicine, and after waking up on the same day, he pulled out the endotracheal tube and walked on the ground the next day. The patient was treated with dual antiplatelets and was successfully discharged from the hospital 6 days after surgery.
Coronary CT angiography evaluation at 1 month postoperatively shows patency of stents of the left anterior descending branch, good aortic valve frame unfolding, no significant thickening of the leaflets, patency of the double coronary artery opening, and ease of later coronary intervention (figure 4).
Patients were followed up 6 months after surgery and had no significant symptoms. Echocardiography suggests that the aortic valve biovalve function is good, with a small amount of perivalular leakage, a peak flow rate of 1.8 m/s, a cross-valve pressure difference of 8 mmHg, and a left ventricular ejection fraction of 62%.
In this case, SinoCrownTM valve was successfully used in China to successfully treat a low-risk surgical patient with severe aortic valve stenosis, and the perioperative operation was safe and feasible, the postoperative follow-up effect was good, and the coronary intervention in the later stage was more convenient.
Source: Chen Yang, Liu Qingrong, Niu Guannan, et al. SinoCrownTM percutaneous interventional aortic valve insertion in China. Chinese Journal of Recycling,2022,32:193-196.] DOI: 10.3969/j.issn.1000-3614.2022.02.014.【Scan QR code to read the full text】
Many difficult and complex cases, a doctor can only see once in a lifetime
Long press the picture to display the recognition QR code, or scan the QR code with your mobile phone to enter the purchase process:
List of recommended brand activities of the National Health Commission
【Chinese Circulation Journal】:This public account is committed to reporting the latest outstanding scientific research results published in academic journals at home and abroad in cardiovascular diseases and related fields, welcome to pay attention to, forward, submit and share, please contact: 18656052587 (WeChat) or [email protected]