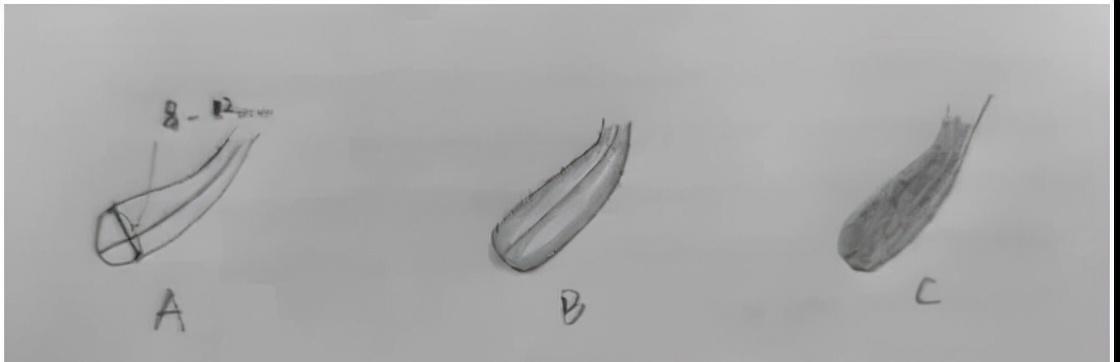
The morphology of the endometrium is roughly divided into a, b, c type, type A endometrium has three linear signs, that is, three clear lines can be seen under ultrasound, and type a endometrium generally appears in the follicle stage, that is, before ovulation. Endometrium type b is generally presented with three lines of thickening and blurring under ultrasound during or shortly after ovulation. Type c intima generally appears before menstruation or during menstruation, and the third line signs are not visible under ultrasound, and the overall echo of the endometrium is strong.
In the natural cycle, the transplant time is generally set after ovulation, and the endometrial form we saw that day may be b-type, at this time it cannot be considered that the lining is not good, on the contrary, after ovulation, the endometrium is converted to b-type, indicating that the endometrial transformation is normal.
In the artificial cycle, ultrasound monitoring is generally done during the follicular stage, so the endometrium seen is mostly type A or a-b type, and then transformed with drugs.

However, in these two transplant cycles, endometrium type C is rarely seen. Type C endometrium appears at an inappropriate stage, embryo transfer is not performed first, the cause should be investigated, if there is no other lesions such as endometrial hyperplasia or inflammation. If the monitoring is still c-type after troubleshooting the cause, transplantation can also be tried.
The best endometrium for embryo implantation is 8-12 mm, < 6 mm (too thin) or > 14 mm (too thick), you should look for reasons.
The intima is too thin, should be combined with estrogen levels, follicle size or drug dose, or whether the endometrium is damaged, if it can be further thickened, should be tried; if it is caused by endometrial damage, the treatment effect is very small, it is difficult to improve the thickness, you can start from improving the blood flow under the endometrium, that is, although the soil is not thick, but make it more fertile, so that the embryo is also promising for planting.
Endometrial hyperplasia, polyps, inflammation, etc. should be excluded, and can be judged by hysteroscopy and endometrial pathological examination, there is a problem with targeted treatment, no problem, then you can transplant.
The optimal endometrial thickness mentioned here is for 95% of people, and 5% of people are not in this range but are normal, and still cannot be compared with others. Rest assured that the decision will be made by your doctor in charge!