Imaging reading techniques have always been a weakness, especially cranial CT! The structure of the skull is complex, the imaging performance is not simple, how to overcome this learning difficulty, I hope this article can help you.
According to the purpose of the study, scans with a certain thickness made along a certain direction, that is, tomographic images, including transverse faults, sagittal positions, and coronal positions. The focus of this article is on ct of the transverse tomum of the skull.
1
A common baseline for cranial tomography
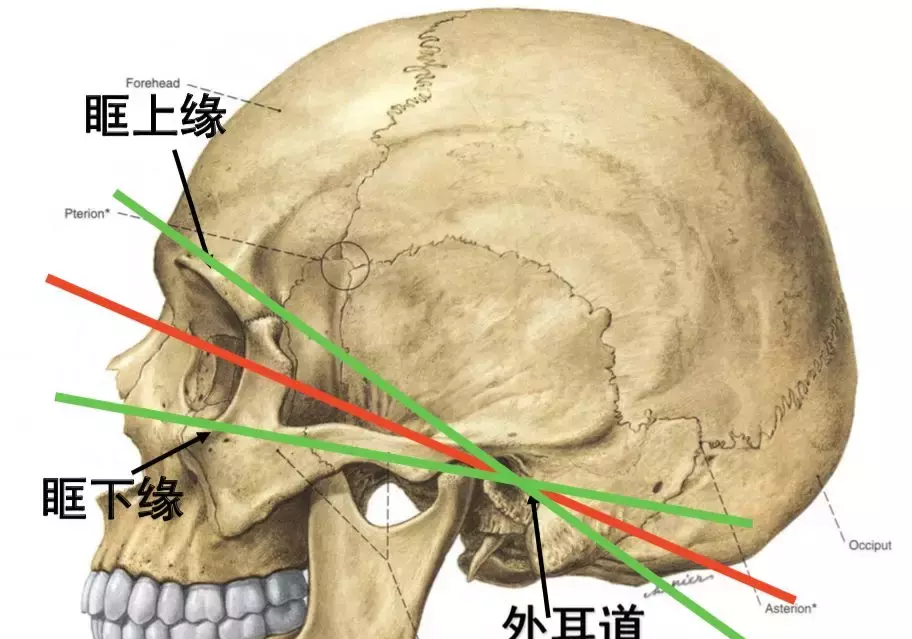
1. Reid baseline (REL): the connection from the midpoint of the external auditory canal to the inferior orbital border. The production of head transverse fault specimens is mostly based on this line, and the production baseline of crown fault specimens is perpendicular to this line.
2. Orbital ear line (OML) or canthal ear line (CML): the connection between the midpoint of the external auditory canal and the external canthus. Cranial axial scans (transverse tomography) are mostly based on this line.
3. Upper orbital ear line (SML): it is the connection between the midpoint of the external auditory canal and the midpoint of the upper orbital margin, and the plane through this line is about the same as the base plane of the skull, which is conducive to showing the posterior fossa structure and reducing skull artifacts.
2
CT window technology
The structure of human tissues is different, the X-ray attenuation is different, and different CT values are formed, so different CT values can be used to identify the nature of tissues.
The absorption of X-ray by air is 0, so the CT value of air is -1000; the X-ray attenuation of bone tissue is 2-4 times that of water, and the CT value of CT is +1000; and the CT value of water is 0.

3
Indications for cranial CT
• Intracranial tumors: meningiomas, gliomas
• Cerebrovascular disease: cerebral hemorrhage, cerebral infarction, subarachnoid hemorrhage
• Head injury: cerebral contusion, hematoma
• Intracranial inflammatory lesions: encephalitis, brain abscess
• Cerebral parasitic diseases: neurocysticercosis
• Congenital malformations and neonatal diseases: neonatal ischemic hypoxic encephalopathy
The following is the key point of this content, which lists the normal imaging performance at all levels of cranial CT, and distinguishing the following is a key step in understanding cranial CT.
The canthal earline level of the subranial surface
(1) Bottom of anterior fossa: orbit, eyeball, sieve sinus, sphenoid sinus, anterior bed process, etc.
(2) Midranial fossa: sphenoid bone --- anterior boundary; posterior boundary --- temporal bone rock part (rock bone); inner margin --- cavernous sinus and pituitary fossa; outer margin --- temporal bone, the temporal lobe in the fossa, and the medial side of which is hippocampal gyrus.
(3) Posterior fossa: the anterior margin --- rock bone; the posterior margin --- occipital bone; the posterior --- anterior pontine pool behind the saddle, extending to both sides as the pontocebellar horn pool.
(4) Fourth ventricle: located on the midline of the posterior fossa, immediately behind the cerebellar worm, flanked by cerebellar tonsils.
(5) Bulbar, pontine: located in front of the fourth ventricle.
Saddle on the pool level
(1) Anterior fossa: temporal lobe.
(2) Saddle upper pool: above the pituitary fossa, between the two sides of the midcranial fossa, the anterior boundary is the temporal lobe straight back, the lateral azimuthoral leaf hippocampus, in the shape of a five-pointed star or hexagonal star. Its anterior angle is connected to the longitudinal fissure pool, the two outer angles are connected to the outer fissure pool, the two posterior lateral angles continue in the ring pool, and the sixth angle is located in the middle of the posterior edge, which is the interangular pool. The edge of the suprasellar pool is a cerebral artery ring, and a "v" optic chircus is often seen in the anterior part of the pool.
(3) Posterior fossa: four ventricles or quadrupletular hydrangea.
The third ventricle at the lower level
(1) The lower part of the anterior angle of the lateral ventricle is shown: the anterior --- frontal lobe; the lateral --- the head of the caudate nucleus; the posterior midline --- the third ventricle, which is connected to the thalamus on both sides.
(2) Posterior fossa: "Y" or "V" shaped cerebellar constellation, the subsurfacea structure is medial (superior cerebellar worm), and the supine structure is lateral (occipital lobe).
(3) Tetragonal pool: located in front of the cerebellar worm.
4
The upper level of the third ventricle
(1) Basal nucleus, thalamus.
(2) The anterior foot (forelimb) of the inner capsule; between the caudal nucleus and the bean-like nucleus.
(3) The knee and hind feet (hind limbs) of the inner capsule are located between the bean-shaped nucleus (composed of the lateral shell nucleus and the medial globule pals) and the thalamus.
(4) Lateral side of the shell nucleus: external capsule, screen nucleus, outermost capsule, insular lobe (instilla).
(5) Tetragonal pool: between the occipital lobes on both sides, there is a pineal gland in the pool, which is connected anteriorly to the third ventricle.
● Basal ganglia (basal nucleus): Gray matter nuclei buried deep in the cerebral hemispheres on both sides, which are the main structures that make up the extrapyramidal system.
Basal node area: the concept is not clear.
May include: basal ganglia, substantia nigra, red nuclei, and the surrounding area of white matter.
● Inner capsule: The white matter area located between the thalamus, caudal nucleus, and bean-like nucleus is densely packed by upper and lower conduction bundles. It is divided into three parts: forelimb, knee, and hindlimb. The knees consist of a cortical brainstem bundle; the hind limbs have a corticospinal tract, a thalamic cortical tract, auditory radiation, and visual radiation.
● External capsule: It is a white matter band located between the screen nucleus and the bean-like nucleus, which is mainly composed of cortical cover fibers emitted by the island leaves.
5
Lateral ventricular body level
It consists of the frontal, temporal, and occipital lobes, with a transparent septum between the ventricles on both sides and a caudal nucleus and body on the outside. The posterior angle of the lateral ventricle (occipital angle) may be asymmetrical, and choroid plexus calcifications may be seen indoors. The longitudinal cleft pool and the brain sickle are visible at the midline.
6
Lateral ventricular upper level
The medial wall side ventricular body part is separated by the callosum, the outer part of the lateral ventricular body part is the parietal lobe, and the parietal sulcus and central sulcus divide the brain into the frontal, apical, and occipital lobes.
7
Lower level of the cerebral cortex (semi-oval central level)
Above the corpus callosum and lateral ventricles, the brain sickle runs from anterior to posterior through the midline. The white matter part is the center of the semi-oval, the frontal lobe is reduced, the proportion of the parietal lobe is enlarged, and the occipital lobe is basically disappeared.
Semi-ovoid center: located above the callosum, myelinated fibers formed by the medulla of the left and right cerebral hemispheres, symmetrically located in the areas on both sides of the brain sickle.
8
Upper level of the cerebral cortex (upper level of the semi-ovary area)
Near the top of the skull, the brain sickle is clearly visible, and the gray matter and sulcus next to it are very clear. The parietal lobes are smaller and the frontal lobes are smaller.
Radiant crown: is the radial fiber white matter between the inner capsule and the cerebral cortex.
The following enters the actual combat drill, proficient in cerebral hemorrhage and cerebral infarction of the skull CT performance, is an essential skill for brain doctors.
Cerebral haemorrhage
• A perforation of the cortical artery ------- lobe hemorrhage
• B bean vein artery --------------- shell nucleus bleeding
• C thalamus through the artery ----------- thalamus hemorrhage
• D-basal artery pontine branch --------- pontine hemorrhage
• Cerebellar or anterior inferior cerebellar artery --- cerebellar hemorrhage
Epidural bleeding
It is divided into acute phase, subacute phase and chronic phase. It can be seen that the subparabin of the skull is fusiform or biconvex with high density, and there may be different degrees of mass effects according to the amount of hematoma, such as loss of the sulcus, deformation of ventricular pressure, and displacement of midline structure. Over time, its density can change from high to equal density to low density.
Subdural hematoma
Acute subdural hematoma: sublarial crescent-shaped high density, often accompanied by cerebral contusion, with obvious mass effect.
Subacute subdural hematoma: crescent-shaped or half-moon-shaped, hematoma density is high-density or isomorphic.
Chronic subdural hematoma: high, low confounding density, and finally becomes low density until it disappears.
Cerebral infarction
According to the anatomical site, it can be divided into:
(1) Cerebral infarction: the --- of large infarction is more than one lobe, more than 5 cm; the --- of medium infarction is less than one lobe of the brain 3-5 cm; the small infarction is 1.6-3 cm; the --- of lacunar infarction is less than 1.5cm; multiple infarction --- multiple small and medium-sized and lacunar infarction.
(2) Cerebellar infarction
(3) Brainstem infarction
This content ends here, the imaging performance of the skull is more complicated, but for complex things, it also has its own routine, "knowing the constant change" and "integrating and penetrating" is the key to mastering knowledge, I hope that this content is helpful to everyone's learning.
Source: Medical Neurology Channel
【Copyright Notice】This platform is a public welfare learning platform, reprinted for the purpose of transmitting more learning information, and has indicated the author and source, such as teachers who do not want to be disseminated can contact us to delete